

Metabolic effects of bariatric surgery in patients with moderate obesity and type 2 diabetes: analysis of a randomized control trial comparing surgery with intensive medical treatment
- PMID: 23439632
- PMCID: PMC3714483
- DOI: 10.2337/dc12-1596
Metabolic effects of bariatric surgery in patients with moderate obesity and type 2 diabetes: analysis of a randomized control trial comparing surgery with intensive medical treatment
Abstract
Objective: To evaluate the effects of two bariatric procedures versus intensive medical therapy (IMT) on β-cell function and body composition.
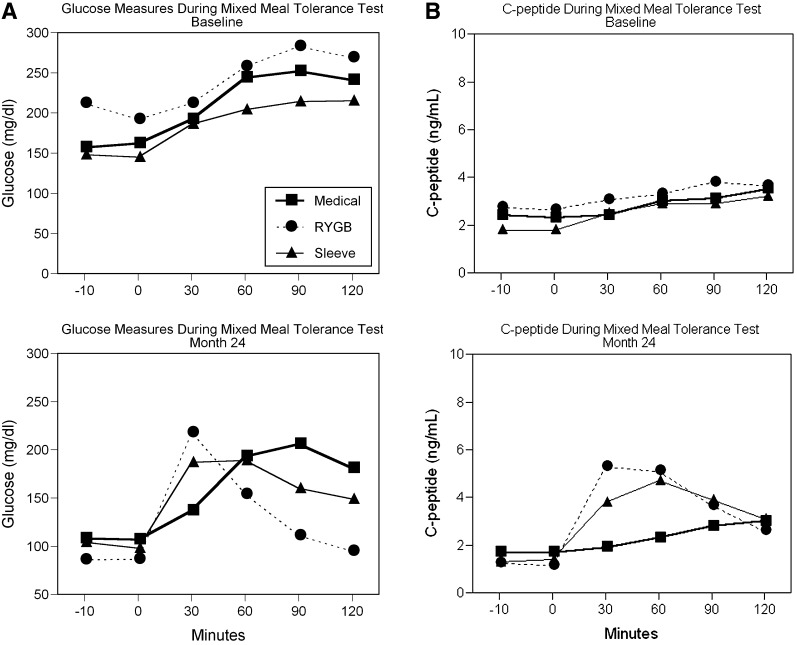
Research design and methods: This was a prospective, randomized, controlled trial of 60 subjects with uncontrolled type 2 diabetes (HbA1c 9.7 ± 1%) and moderate obesity (BMI 36 ± 2 kg/m(2)) randomized to IMT alone, IMT plus Roux-en-Y gastric bypass, or IMT plus sleeve gastrectomy. Assessment of β-cell function (mixed-meal tolerance testing) and body composition was performed at baseline and 12 and 24 months.
Results: Glycemic control improved in all three groups at 24 months (N = 54), with a mean HbA1c of 6.7 ± 1.2% for gastric bypass, 7.1 ± 0.8% for sleeve gastrectomy, and 8.4 ± 2.3% for IMT (P < 0.05 for each surgical group versus IMT). Reduction in body fat was similar for both surgery groups, with greater absolute reduction in truncal fat in gastric bypass versus sleeve gastrectomy (-16 vs. -10%; P = 0.04). Insulin sensitivity increased significantly from baseline in gastric bypass (2.7-fold; P = 0.004) and did not change in sleeve gastrectomy or IMT. β-Cell function (oral disposition index) increased 5.8-fold in gastric bypass from baseline, was markedly greater than IMT (P = 0.001), and was not different between sleeve gastrectomy versus IMT (P = 0.30). At 24 months, β-cell function inversely correlated with truncal fat and prandial free fatty acid levels.
Conclusions: Bariatric surgery provides durable glycemic control compared with intensive medical therapy at 2 years. Despite similar weight loss as sleeve gastrectomy, gastric bypass uniquely restores pancreatic β-cell function and reduces truncal fat, thus reversing the core defects in diabetes.
Trial registration: ClinicalTrials.gov NCT00432809.
Figures
References
-
- Danaei G, Finucane MM, Lu Y, et al. ; Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Blood Glucose) National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet 2011;378:31–40 - PubMed
-
- Buchwald H, Oien DM. Metabolic/bariatric surgery Worldwide 2008. Obes Surg 2009;19:1605–1611 - PubMed
-
- Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med 2012;366:1577–1585 - PubMed
-
- Gatmaitan P, Huang H, Talarico J, et al. Pancreatic islet isolation after gastric bypass in a rat model: technique and initial results for a promising research tool. Surg Obes Relat Dis 2010;6:532–537 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
