

Dynamic neuromuscular stabilization & sports rehabilitation
- PMID: 23439921
- PMCID: PMC3578435
Dynamic neuromuscular stabilization & sports rehabilitation
Abstract
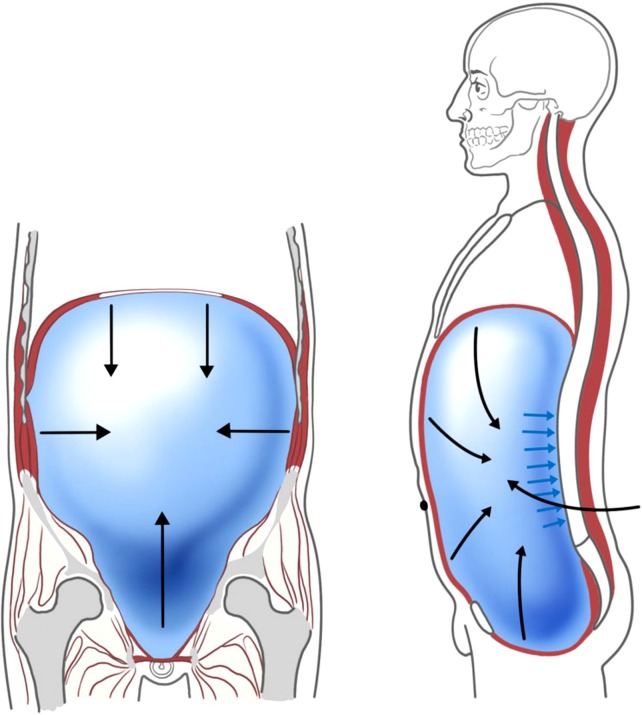
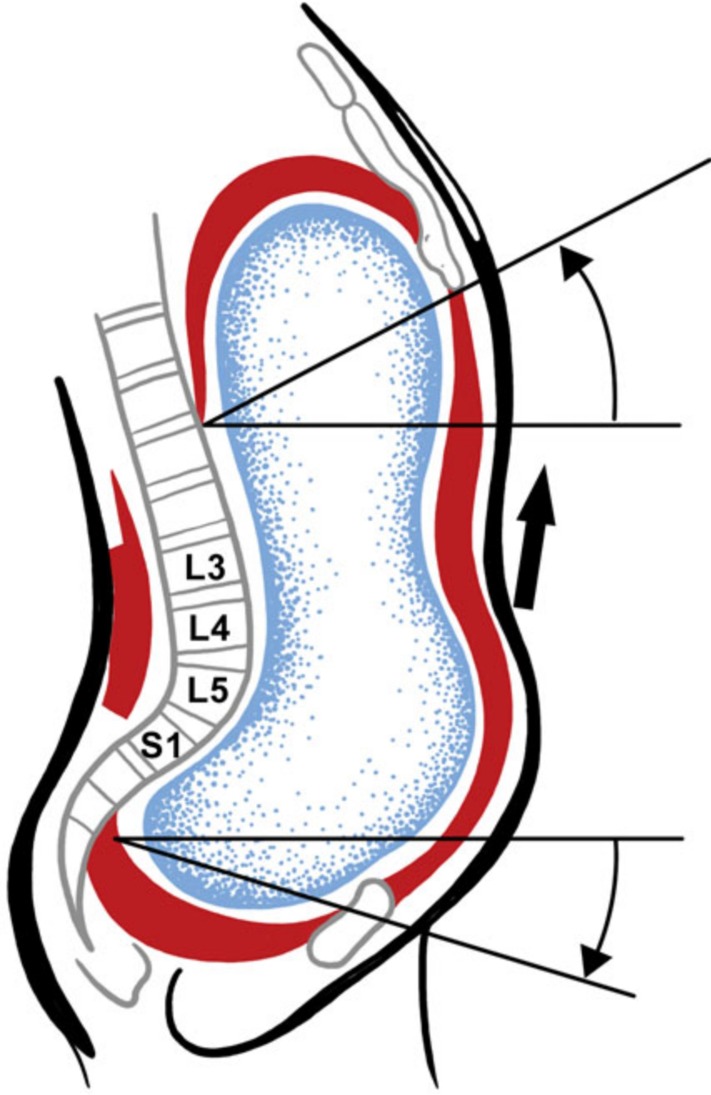
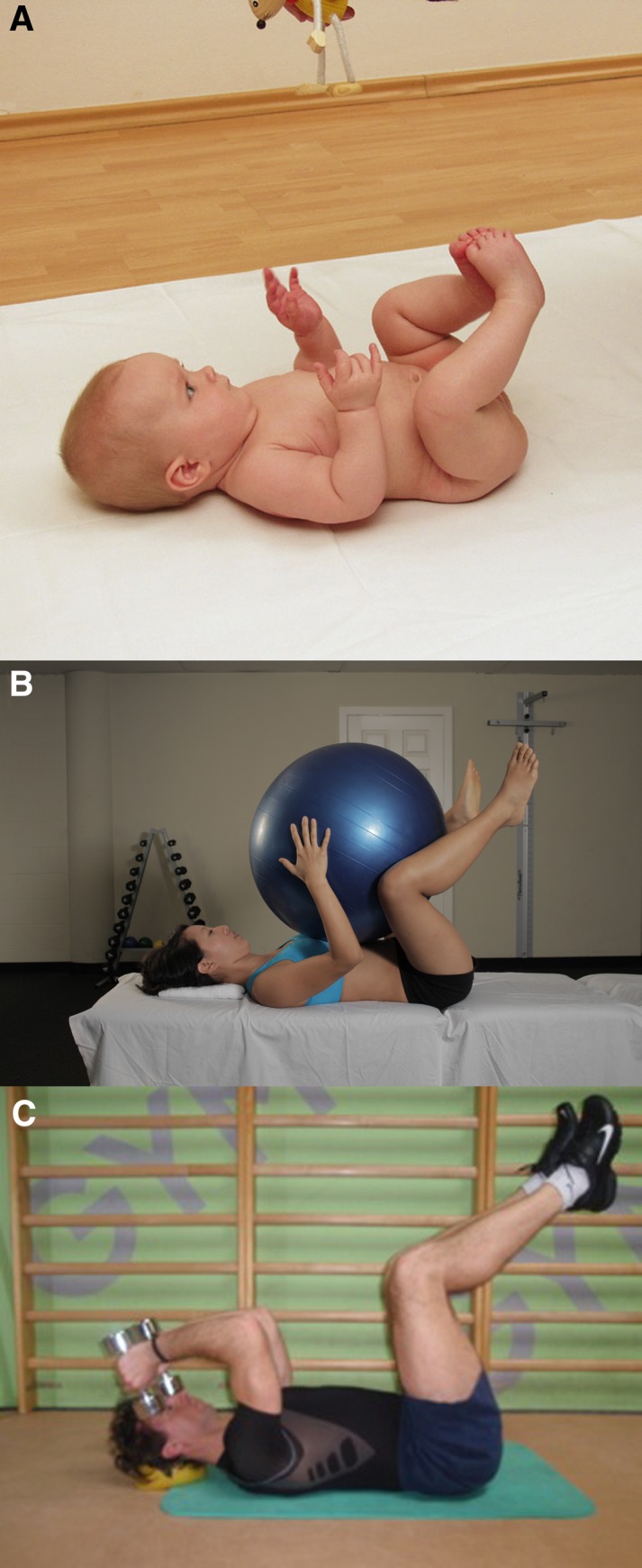
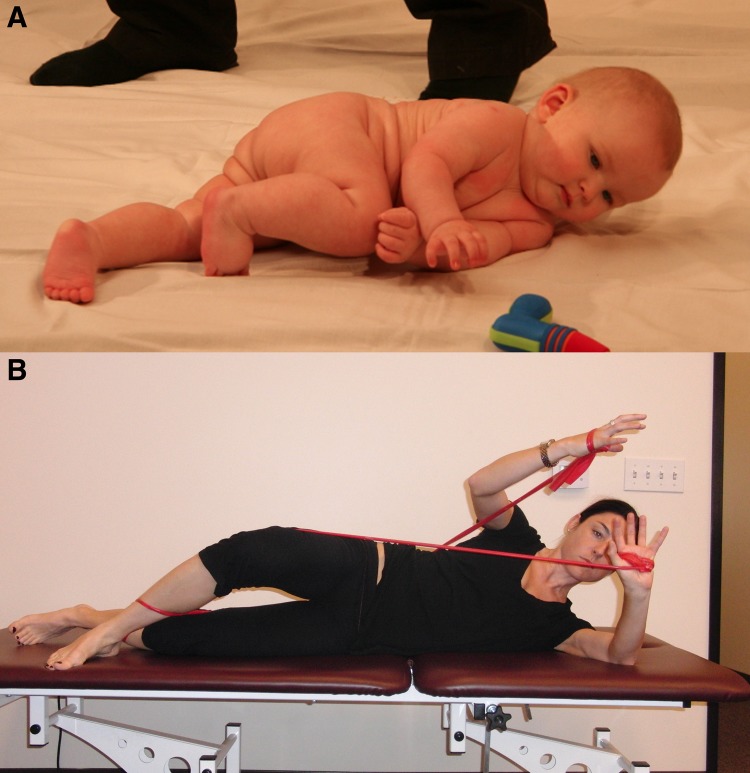
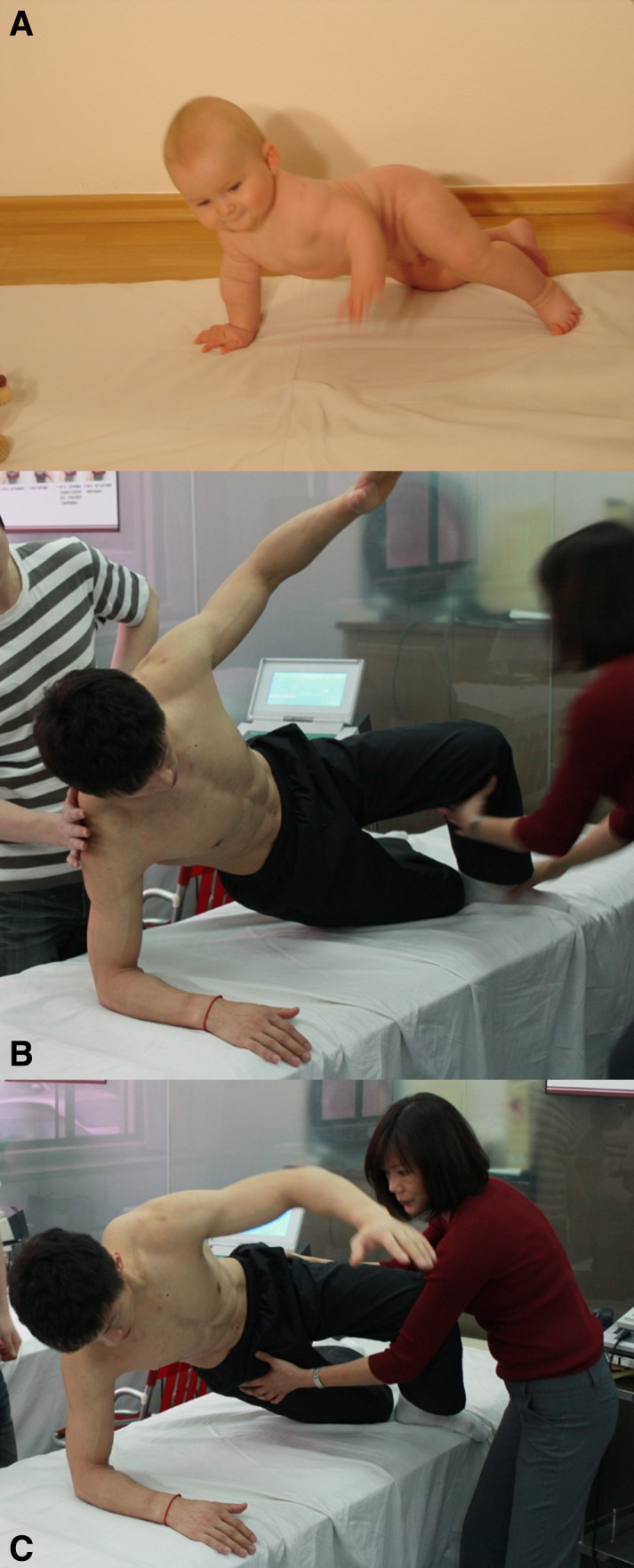
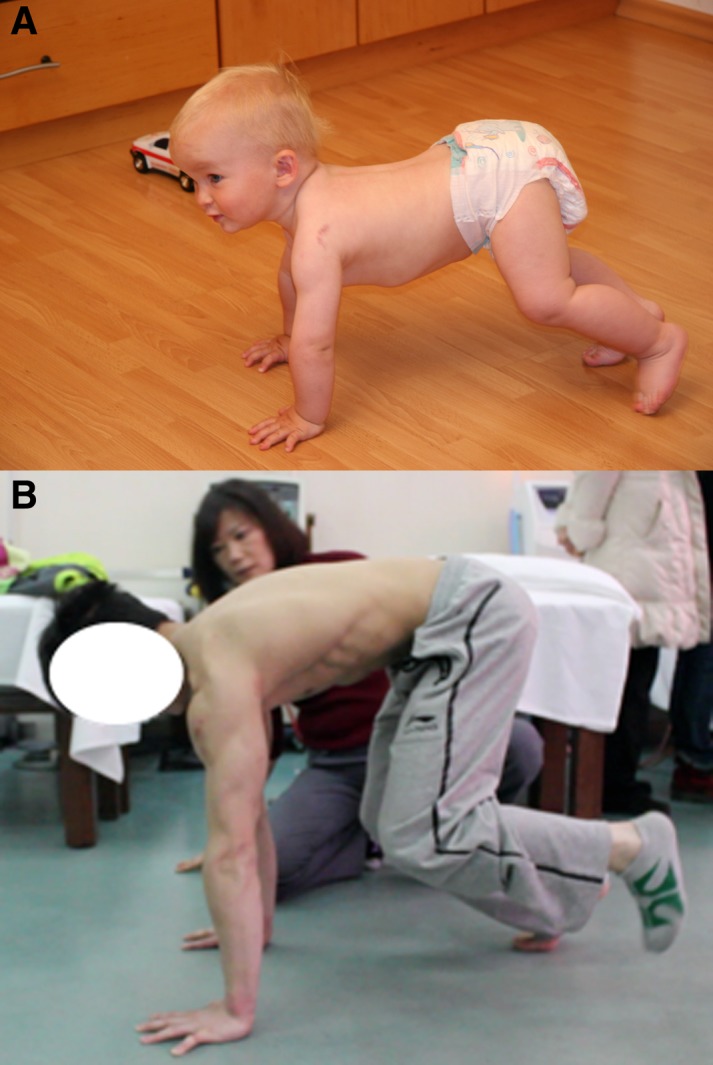
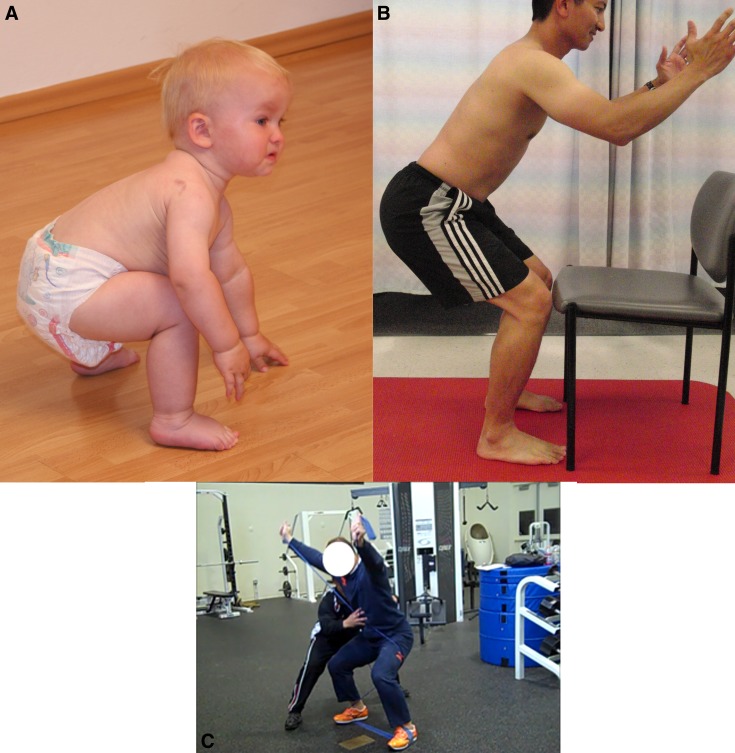
Dynamic neuromuscular (core) stability is necessary for optimal athletic performance and is not achieved purely by adequate strength of abdominals, spinal extensors, gluteals or any other musculature; rather, core stabilization is accomplished through precise coordination of these muscles and intra-abdominal pressure regulation by the central nervous system. Understanding developmental kinesiology provides a framework to appreciate the regional interdependence and the inter-linking of the skeleton, joints, musculature during movement and the importance of training both the dynamic and stabilizing function of muscles in the kinetic chain. The Dynamic Neuromuscular Stabilization (DNS) approach provides functional tools to assess and activate the intrinsic spinal stabilizers in order to optimize the movement system for both pre-habilitation and rehabilitation of athletic injuries and performance.
Level of evidence: 5.
Keywords: Core stabilization; developmental kinesiology; dynamic neuromuscular stabilization; integrated spinal stabilizing system.
Figures



References
-
- Cholewicki J, Juluru K, McGill SM. Intra-abdominal pressure mechanism for stabilizing the lumbar spine. J. Biomech. 1999a;32(1):13–17 - PubMed
-
- Cresswell AG, Grundström H, Thorstensson A. Observations on intra-abdominal pressure and patterns of abdominal intra-muscular activity in man. Acta Physiol. Scand. 1992;144(4):409–18 - PubMed
-
- Gardner‐Morse MG, Stokes IAF. The effects of abdominal muscle co-activation on lumbar spinestability. Spine. 1998;23(1):86–92 - PubMed
-
- Hodges PW, Eriksson AE, Shirley D, et al. Intra-abdominal pressure increases stiffness of the lumbar spine. J Biomech. 2005;38(9):1873–80 - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials