

CT findings of pulmonary non-tuberculous mycobacterial infection in non-AIDS immunocompromised patients: a case-controlled comparison with immunocompetent patients
- PMID: 23440166
- PMCID: PMC3635784
- DOI: 10.1259/bjr.20120209
CT findings of pulmonary non-tuberculous mycobacterial infection in non-AIDS immunocompromised patients: a case-controlled comparison with immunocompetent patients
Abstract
Objective: To describe CT findings of non-tuberculous mycobacteria (NTM) pulmonary infection in non-AIDS immunocompromised patients (ICPs) and to compare these findings with those in immunocompetent patients.
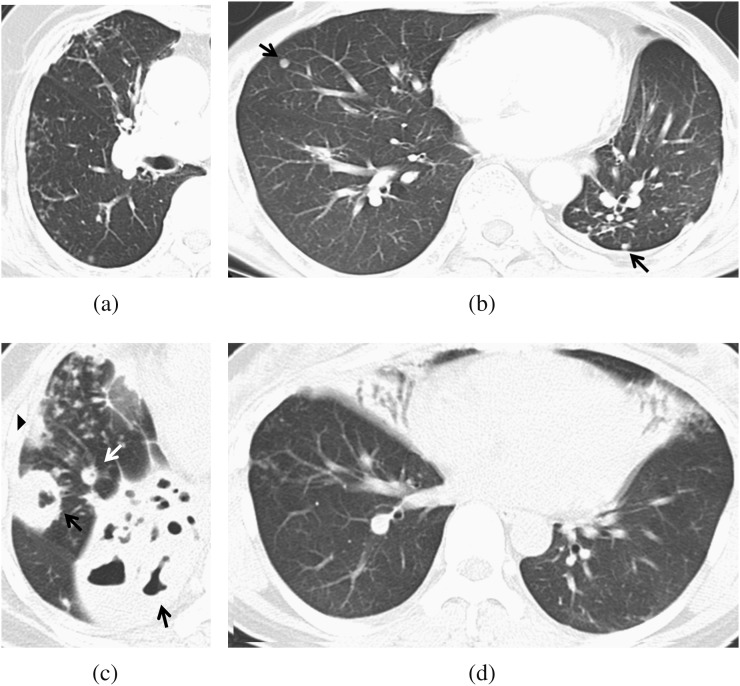
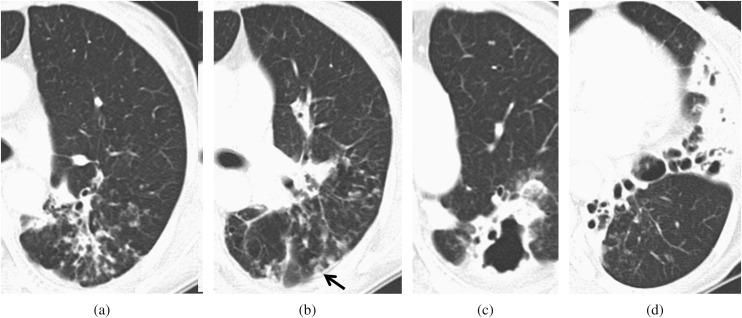
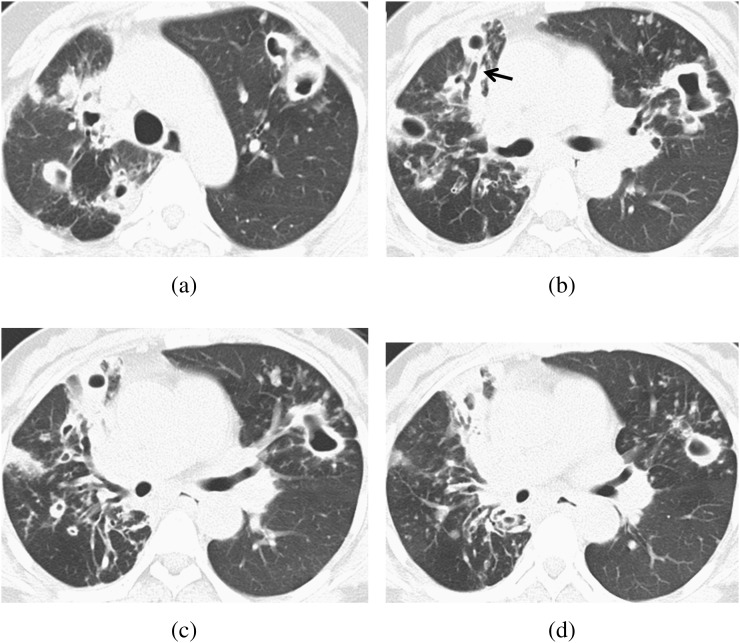
Methods: From July 2000 to August 2007, 369 patients (mean age 58.3 years; 169 males and 200 females) with pulmonary NTM infection were retrospectively reviewed. Of these 369 patients, 24 ICPs (mean age 64.8 years; 15 males and 9 females) were identified. 16 patients had diabetes mellitus, and 6 patients had received long-term steroid therapy. One had received solid organ transplantation and one had received high-dose chemotherapy for haematological disease. 24 age- and sex-matched immunocompetent patients (mean age 64.6 years; 15 males and 9 females) were selected as the control group from the same registry. CT images were reviewed in consensus by three chest radiologists, who were blinded to immune status. Each lung lobe was evaluated in terms of extent of the lesion, bronchiectasis, parenchymal opacity and the presence of ancillary findings. results: A total of 287 lobes were evaluated in ICPs and the control group. The ICPs showed a higher prevalence of ill-defined nodules, with cavities and large opacity >2 cm with/without cavity (p=0.03, 0.04 and 0.02, respectively). Regardless of the immune status, the most common CT findings were bronchiectasis and ill-defined nodules without cavity.
Conclusion: The most common CT findings of pulmonary NTM infection in ICPs were bronchiectasis and ill-defined nodules, similar to those in the control group. Ill-defined nodules with cavity and large opacity >2 cm with/without cavity were more frequently found in ICPs.
Advances in knowledge: In patients affected by NTM infection, large opacities and cavitation in pulmonary nodules are more frequent in ICPs than in immunocompetent patients.
Figures
Similar articles
-
Comparison of chest CT findings in nontuberculous mycobacterial diseases vs. Mycobacterium tuberculosis lung disease in HIV-negative patients with cavities.PLoS One. 2017 Mar 27;12(3):e0174240. doi: 10.1371/journal.pone.0174240. eCollection 2017. PLoS One. 2017. PMID: 28346488 Free PMC article.
-
Nontuberculous mycobacterial pulmonary infection in immunocompetent patients: comparison of thin-section CT and histopathologic findings.Radiology. 2004 Jun;231(3):880-6. doi: 10.1148/radiol.2313030833. Epub 2004 Apr 29. Radiology. 2004. PMID: 15118112
-
Nontuberculous mycobacterial pulmonary infection in patients with idiopathic interstitial pneumonias: comparison with patients without idiopathic interstitial pneumonias.J Comput Assist Tomogr. 2014 Nov-Dec;38(6):972-8. doi: 10.1097/RCT.0000000000000144. J Comput Assist Tomogr. 2014. PMID: 25162293
-
Nontuberculous mycobacterial pulmonary diseases in immunocompetent patients.Korean J Radiol. 2002 Jul-Sep;3(3):145-57. doi: 10.3348/kjr.2002.3.3.145. Korean J Radiol. 2002. PMID: 12271159 Free PMC article. Review.
-
Interrelational changes in the epidemiology and clinical features of nontuberculous mycobacterial pulmonary disease and tuberculosis in a referral hospital in Japan.Respir Med. 2019 Jun;152:74-80. doi: 10.1016/j.rmed.2019.05.001. Epub 2019 May 8. Respir Med. 2019. PMID: 31128614 Review.
Cited by
-
Clinical significance of nontuberculous mycobacteria from respiratory specimens in stem cell transplantation recipients.Int J Hematol. 2015 May;101(5):505-13. doi: 10.1007/s12185-015-1745-9. Epub 2015 Feb 8. Int J Hematol. 2015. PMID: 25663510
-
Pulmonary Mycobacterium avium infection demonstrating unusual lobar caseous pneumonia.Respirol Case Rep. 2016 Jul 5;4(5):e00176. doi: 10.1002/rcr2.176. eCollection 2016 Sep. Respirol Case Rep. 2016. PMID: 27516892 Free PMC article.
-
Characteristics associated with progression in patients with of nontuberculous mycobacterial lung disease : a prospective cohort study.BMC Pulm Med. 2017 Jan 5;17(1):5. doi: 10.1186/s12890-016-0349-3. BMC Pulm Med. 2017. PMID: 28056937 Free PMC article.
-
Can physics principles help explain why non-tuberculous mycobacterial lung disease is more severe in the right middle lobe and lingula?J Thorac Dis. 2019 Nov;11(11):4847-4854. doi: 10.21037/jtd.2019.10.70. J Thorac Dis. 2019. PMID: 31903275 Free PMC article. No abstract available.
-
The Differential Diagnostic Value of Chest Computed Tomography for the Identification of Pathogens Causing Pulmonary Infections in Patients with Hematological Malignancies.Infect Drug Resist. 2024 Oct 21;17:4557-4566. doi: 10.2147/IDR.S474229. eCollection 2024. Infect Drug Resist. 2024. PMID: 39464837 Free PMC article.
References
-
- O'Brien RJ, Geiter LJ, Snider DE., Jr The epidemiology of nontuberculous mycobacterial diseases in the United States. Results from a national survey. Am Rev Respir Dis 1987;135:1007–14 - PubMed
-
- Wolinsky E. Nontuberculous mycobacteria and associated diseases. Am Rev Respir Dis 1979;119:107–59 - PubMed
-
- Diagnosis and treatment of disease caused by nontuberculous mycobacteria. Am Rev Respir Dis 1990;142:940–53 - PubMed
-
- Diagnosis and treatment of disease caused by nontuberculous mycobacteria. This official statement of the American Thoracic Society was approved by the Board of Directors, March 1997. Medical Section of the American Lung Association. Am J Respir Crit Care Med 1997;156:S1–25 - PubMed
-
- Runyon EH. Anonymous mycobacteria in pulmonary disease. Med Clin North Am 1959;43:273–90 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
