

Ask-Advise-Connect: a new approach to smoking treatment delivery in health care settings
- PMID: 23440173
- PMCID: PMC3858085
- DOI: 10.1001/jamainternmed.2013.3751
Ask-Advise-Connect: a new approach to smoking treatment delivery in health care settings
Abstract
Importance: Several national health care-based smoking cessation initiatives have been recommended to facilitate the delivery of evidence-based treatments, such as quitline (telephone-based tobacco cessation services) assistance. The most notable examples are the 5 As (Ask, Advise, Assess, Assist, Arrange) and Ask. Advise. Refer. (AAR) programs. Unfortunately, rates of primary care referrals to quitlines are low, and most referred smokers fail to call for assistance.
Objective: To evaluate a new approach--Ask-Advise-Connect (AAC)--designed to address barriers to linking smokers with treatment.
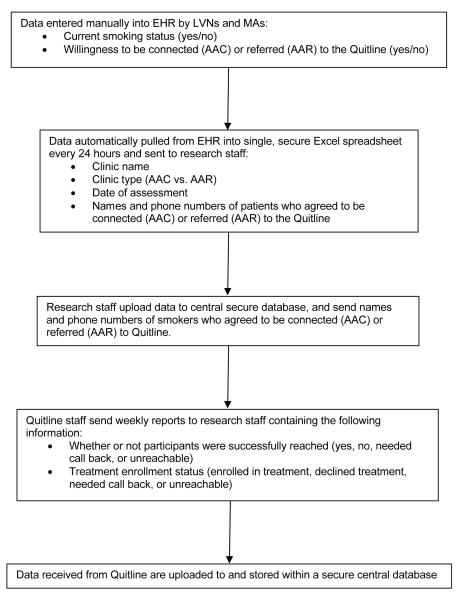
Design: A pair-matched, 2-treatment-arm, group-randomized design in 10 family practice clinics in a single metropolitan area. Five clinics were randomized to the AAC (intervention) and 5 to the AAR (control) conditions. In both conditions, clinic staff were trained to assess and record the smoking status of all patients at all visits in the electronic health record, and smokers were given brief advice to quit. In the AAC clinics, the names and telephone numbers of smokers who agreed to be connected were sent electronically to the quitline daily, and patients were called proactively by the quitline within 48 hours. In the AAR clinics, smokers were offered a quitline referral card and encouraged to call on their own. All data were collected from February 8 through December 27, 2011.
Setting: Ten clinics in Houston, Texas.
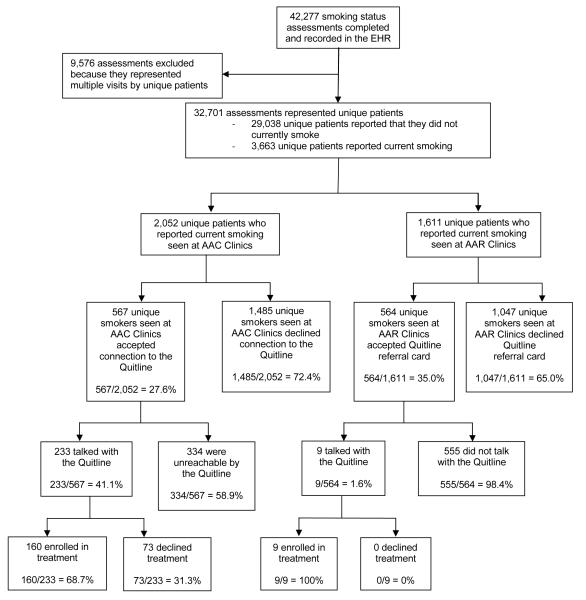
Participants: Smoking status assessments were completed for 42,277 patients; 2052 unique smokers were identified at AAC clinics, and 1611 smokers were identified at AAR clinics.
Interventions: Linking smokers with quitline-delivered treatment.
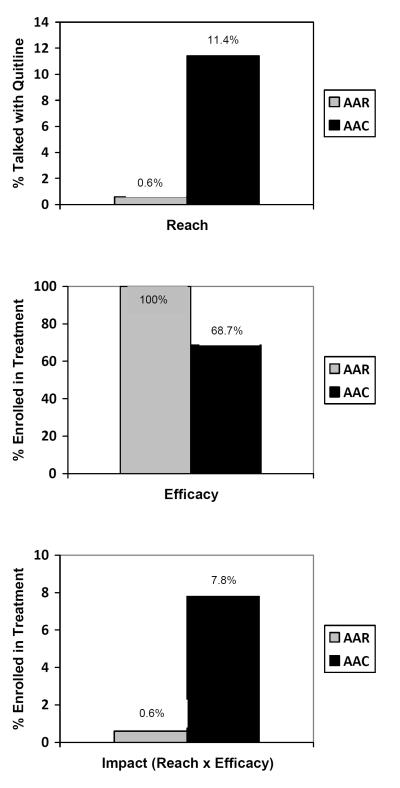
Main outcome measure: Impact was based on the RE-AIM (Reach, Efficacy, Adoption, Implementation, and Maintenance) conceptual framework and defined as the proportion of all identified smokers who enrolled in treatment.
Results: In the AAC clinics, 7.8% of all identified smokers enrolled in treatment vs 0.6% in the AAR clinics (t4 = 9.19 [P < .001]; odds ratio, 11.60 [95% CI, 5.53-24.32]), a 13-fold increase in the proportion of smokers enrolling in treatment.
Conclusions and relevance: The system changes implemented in the AAC approach could be adopted broadly by other health care systems and have tremendous potential to reduce tobacco-related morbidity and mortality.
Figures
Comment in
-
The quitline is calling: comment on "Ask-Advise-Connect".JAMA Intern Med. 2013 Mar 25;173(6):464. doi: 10.1001/jamainternmed.2013.4086. JAMA Intern Med. 2013. PMID: 23440224 No abstract available.
References
-
- Adami HO, Day NE, Trichopoulos D, Willett WC. Primary and secondary prevention in the reduction of cancer morbidity and mortality. Eur J Cancer. 2001;37(Suppl 8):S118–27. - PubMed
-
- CDC Cigarette smoking among adults-United States, 2003. MMWR Morb Mortal Wkly Rep. 2005;54:509–13. - PubMed
-
- Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. Journal of the American Medical Association. 2004;291:1238–45. - PubMed
-
- McGinnis JM, Foege WH. Actual causes of death in the United States. Journal of the American Medical Association. 1993;270:2207–12. - PubMed
-
- USDHHS . The Health Benefits of Smoking Cessation. In: Service PH, editor. A Report of the Surgeon General. Vol. 1990. Centers for Disease Control and Prevention, Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 1990.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
