

Dilatation of the ascending aorta in patients with congenitally bicuspid aortic valves
- PMID: 23440752
- PMCID: PMC3484928
Dilatation of the ascending aorta in patients with congenitally bicuspid aortic valves
Abstract
Introduction: The cause of ascending aortic dilatation occurring in patients with congenitally bicuspid aortic valves was investigated.
Methods: Flow patterns through human aortic roots with congenitally bicuspid aortic valves as well as through porcine constricted aortas were studied in a left heart simulator. Vibration was recorded as a measure of turbulence in the post-stenotic segment. Histological changes in fetal aortas with isolated congenitally bicuspid aortic valves were compared to fetal aortas with congenitally bicuspid aortic valves and hypoplastic left hearts, as well as to normal fetal aortas with tricuspid aortic valves.
Results: Congenitally bicuspid aortic valves were anatomically stenotic even in the absence of pressure gradients and without history of relevant symptoms. Histology of the aortic wall in isolated fetal congenitally bicuspid aortic valves was similar to that of fetal aortas with normal tri-leaflet aortic valves, but was abnormal if congenitally bicuspid aortic valves was associated with other cardiovascular anomalies. Flow studies revealed that turbulence and vibration in the post-stenotic aortic segments generated by the stenosis were proportional to the degree of the narrowing.
Conclusions: Congenitally bicuspid aortic valves are inherently stenotic, asymmetrical, generate turbulence and vibration. This not only leads to early failure but also to injury of the ascending aortic wall and ascending aortic dilatation. The more progressive form of ascending aortic dilatation occurs in patients where congenitally bicuspid aortic valves is combined with other inborn anomalies and may require a radical procedure (replacement).
Keywords: aortic aneurysm; bicuspid aortic valve.
Conflict of interest statement
Figures



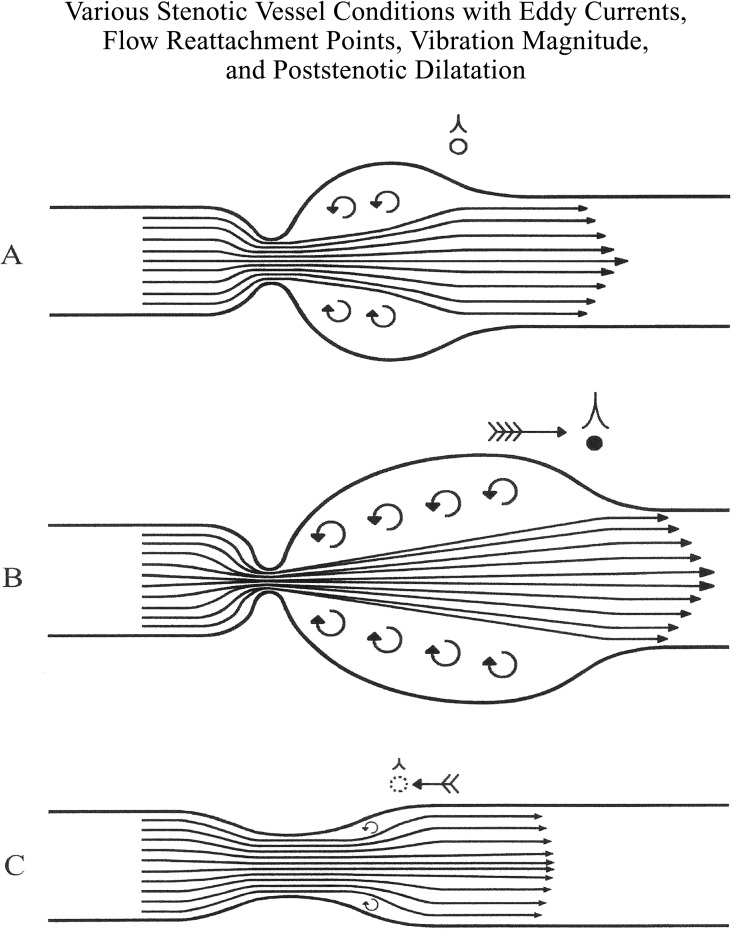
The initial jet flow through the stenosis.
The development of a recirculation zone.
The region of reattachment to the aortic wall.






Hematoxylin eosin stain.
Movat pentachrome stain.
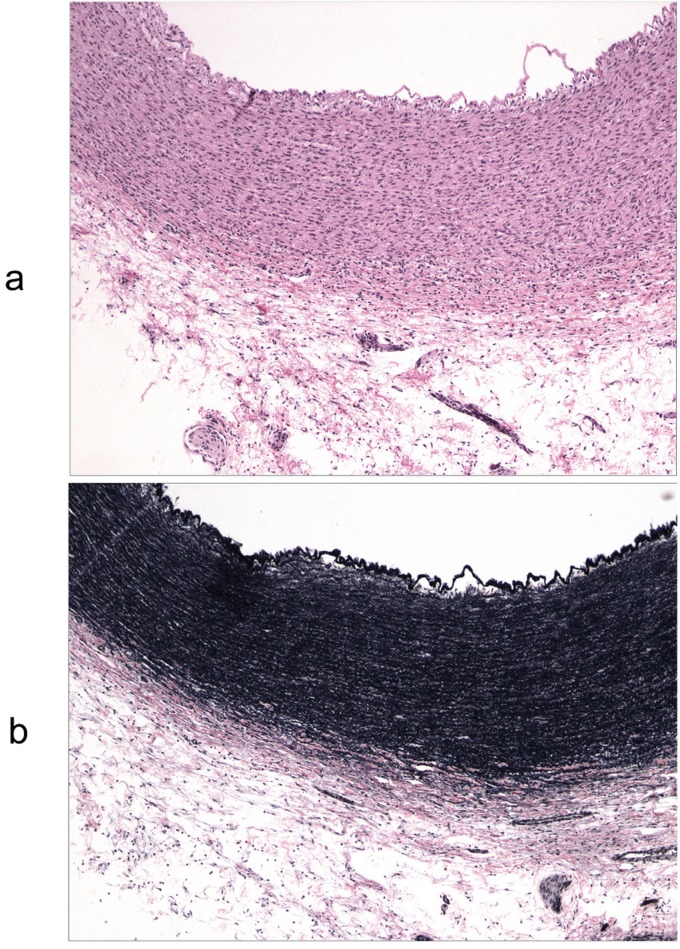
Hematoxylin eosin stain.
Movat pentachrome stain.

Hematoxylin eosin stain.
Movat pentachrome stain.

References
-
- Roberts W C. The congenitally bicuspid aortic valve. A study of 85 autopsy cases. Am J Cardiol. 1970;26:72–83. - PubMed
-
- Roberts W C. The structure of the aortic valve in clinically isolated aortic stenosis: an autopsy study of 162 patients over 15 years of age. Circulation. 1970;42:91–97. - PubMed
-
- Larson E W, Edwards W D. Risk factors for aortic dissection: a necropsy study of 161 cases. Am J Cardiol. 1984;53:849–855. - PubMed
-
- Stewart W J, King M E, Gilliam L D. et al. Prevalence of aortic valve prolapse with bicuspid aortic valve and its relation to aortic regurgitation: a cross-sectional echocardiographic study. Am J Cardiol 1984; 54: 1277-82. 1984;54:1277–1282. - PubMed
-
- Kuralay E, Demirkilic U, Ozal E. et al. Surgical approach to ascending aorta in bicuspid aortic valve. J Card Surg 2003; 18: 173-80. 2003;18:173–180. - PubMed
LinkOut - more resources
Full Text Sources