

Cervical assessment by ultrasound for preventing preterm delivery
- PMID: 23440813
- PMCID: PMC6464944
- DOI: 10.1002/14651858.CD007235.pub3
Cervical assessment by ultrasound for preventing preterm delivery
Update in
-
Cervical assessment by ultrasound for preventing preterm delivery.Cochrane Database Syst Rev. 2019 Sep 25;9(9):CD007235. doi: 10.1002/14651858.CD007235.pub4. Cochrane Database Syst Rev. 2019. PMID: 31553800 Free PMC article.
Abstract
Background: Measurement of cervical length (CL) by transvaginal ultrasound (TVU) is predictive of preterm birth (PTB). It is unclear if this screening test is effective for prevention of PTB.
Objectives: To assess the effectiveness of antenatal management based on transvaginal ultrasound of cervical length (TVU CL) screening for preventing PTB.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 August 2012), reviewed the reference lists of all articles and contacted experts in the field for additional and ongoing trials.
Selection criteria: Published and unpublished randomized controlled trials including pregnant women between the gestational ages of 14 to 32 weeks screened with TVU CL for risk of PTB. This review focuses exclusively on studies based on knowledge versus no knowledge of TVU CL results.
Data collection and analysis: All potential studies identified from the search were independently assessed for inclusion by three review authors. We also analyzed studies for quality measures and extracted data.
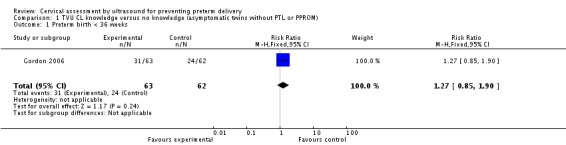
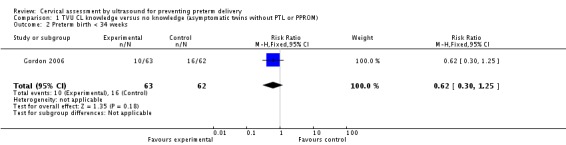
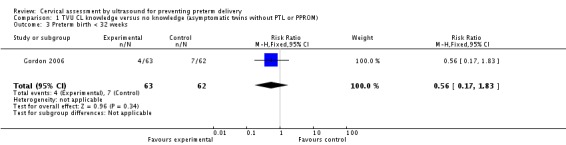
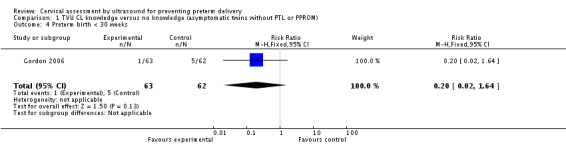
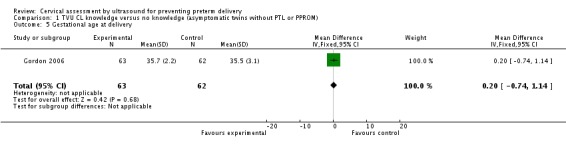
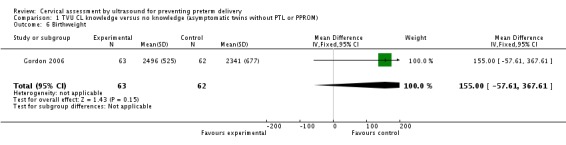
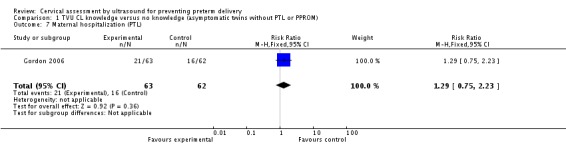
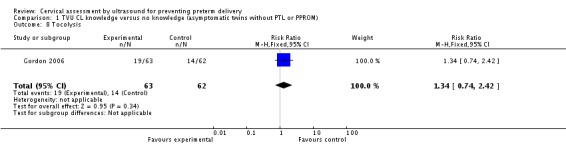
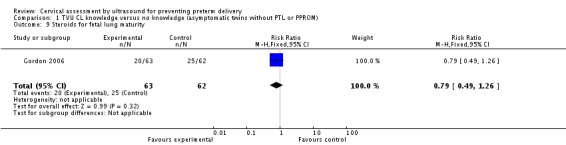
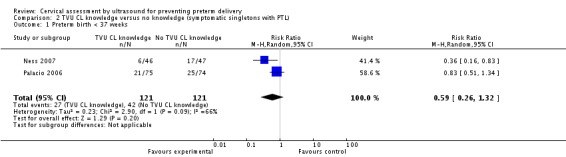
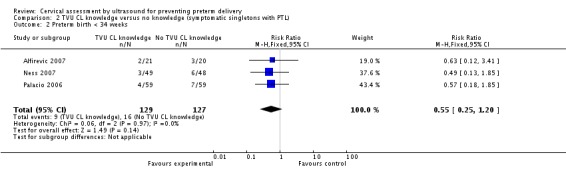
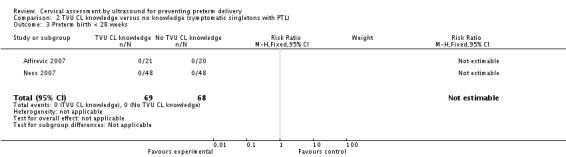
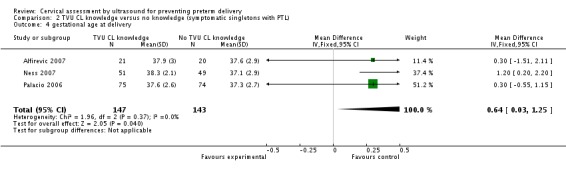
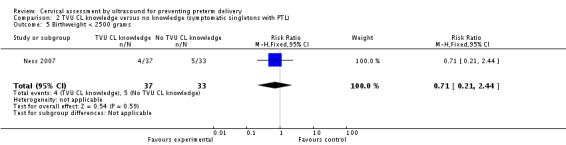
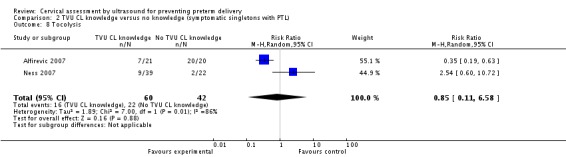
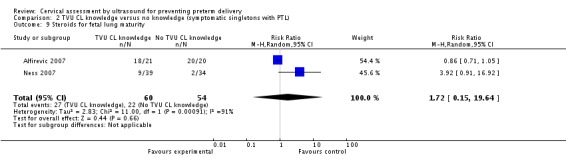
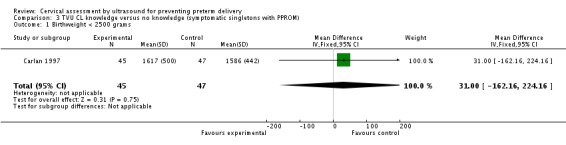
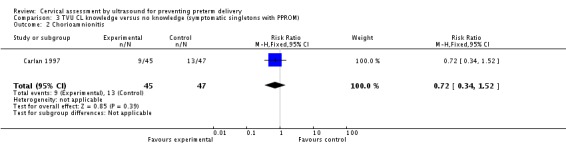
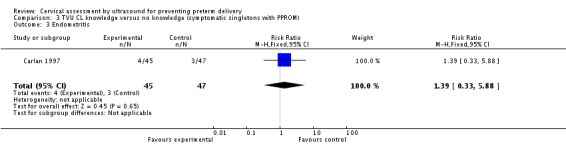
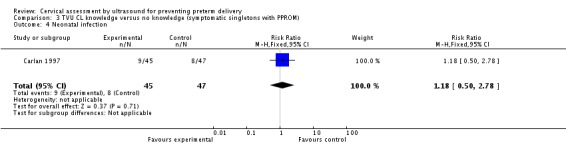
Main results: Of the 13 trials identified, five were eligible for inclusion (n = 507). Three included singleton gestations with preterm labor (PTL); one included singleton gestations with preterm premature rupture of membranes (PPROM); and one included twin gestations with or without PTL.In the three trials of singleton gestations with PTL, 290 women were randomized; 147 to knowledge and 143 to no knowledge of TVU CL. Knowledge of TVU CL results was associated with a non-significant decrease in PTB at less than 37 weeks (22.3% versus 34.7%, respectively; average risk ratio 0.59, 95% confidence interval (CI) 0.26 to 1.32; two trials, 242 women) and at less than 34 weeks (6.9% verus 12.6%; RR 0.55, 95% CI 0.25 to 1.20; three trials, 256 women). Delivery occurred at a later gestational age in the knowledge versus no knowledge groups (mean difference (MD) 0.64 weeks, 95% CI 0.03 to 1.25; three trials, 290 women). For all other outcomes for which there were available data (PTB at less than 34 or 28 weeks; birthweight less than 2500 grams; perinatal death; maternal hospitalization; tocolysis; and steroids for fetal lung maturity), there was no evidence of a difference between groups.The trial of singleton gestations with PPROM (n = 92) evaluated as its primary outcome safety of TVU CL in this population, and not its effect on management. There was no evidence of a difference in incidence of maternal and neonatal infections between the TVU CL and no TVU CL groups.In the trial of twin gestations with or without PTL (n = 125), there was no evidence of a difference in PTB at less than 36, 34, or 30 weeks, gestational age at delivery, and other perinatal and maternal outcomes between the TVU CL and the no TVU CL groups. Life-table analysis revealed significantly less PTB at less than 35 weeks in the TVU CL group compared with the no TVU CL group (P = 0.02).
Authors' conclusions: Currently, there is insufficient evidence to recommend routine screening of asymptomatic or symptomatic pregnant women with TVU CL. Since there is a non-significant association between knowledge of TVU CL results and a lower incidence of PTB at less than 37 weeks in symptomatic women, we encourage further research. Future studies should look at specific populations separately (e.g., singleton versus twins; symptoms of PTL or no such symptoms), report on all pertinent maternal and perinatal outcomes, and include cost-effectiveness analyses. Most importantly, future studies should include a clear protocol for management of women based on TVU CL results, so that it can be easily evaluated and replicated.
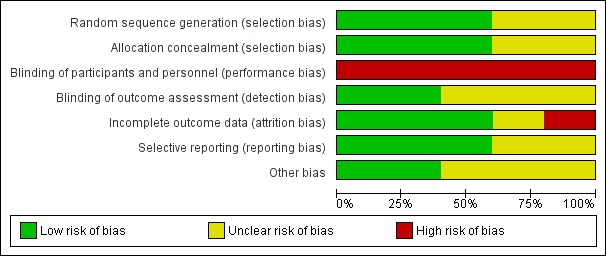
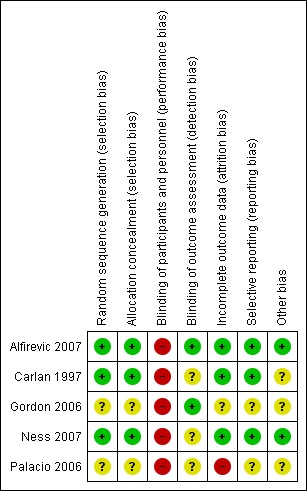
Conflict of interest statement
One of the authors of this Cochrane Review (Vincenzo Berghella) is a co‐author on one of the included trials (Ness 2007).
Figures
Update of
-
Cervical assessment by ultrasound for preventing preterm delivery.Cochrane Database Syst Rev. 2009 Jul 8;(3):CD007235. doi: 10.1002/14651858.CD007235.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2013 Jan 31;(1):CD007235. doi: 10.1002/14651858.CD007235.pub3. PMID: 19588421 Free PMC article. Updated.
References
References to studies included in this review
-
- Alfirevic Z, Allen‐Coward H, Molina F, Vinuesa CP, Nicolaides K. Targeted therapy for threatened preterm labor based on sonographic measurement of the cervical length: a randomized controlled trial. Ultrasound in Obstetrics & Gynecology 2007;29(1):47‐50. - PubMed
-
- Carlan SJ, Richmond LB, O'Brien WF. Randomized trial of endovaginal ultrasound in preterm premature rupture of membranes. Obstetrics & Gynecology 1997;89:458‐61. - PubMed
-
- Gordon M, Robbins A, McKenna D, Howard B, Barth W. Cervical length assessment as a resource to identify twins at risk for preterm delivery (clarity study). American Journal of Obstetrics and Gynecology 2006;195(6 Suppl 1):S55.
-
- Ness A, Visintine J, Ricci E, Berghella V. Does knowledge of cervical length and fetal fibronectin affect management of women with threatened preterm labor? A randomized trial. American Journal of Obstetrics and Gynecology 2007;197(4):426.e1‐426.e7. - PubMed
- Ness A, Visintine J, Ricci E, Boyle K, Berghella V. Use of fetal fibronectin and transvaginal ultrasound cervical length to triage women with suspected preterm labor: a randomized trial. American Journal of Obstetrics and Gynecology 2006;195(6 Suppl 1):S67. - PubMed
-
- Palacio M, Sanchez M, Cobo T, Figueras F, Coll O, Cararach V. Uterine cervical length to reduce length of stay in patients admitted because of preterm labor. Prospective and randomized trial. Preliminary results. Ultrasound in Obstetrics & Gynecology 2003;22(Suppl 1):47.
- Palacio M, Sanchez M, Cobo T, Figueras F, Coll O, Cararach V, et al. Cervical length measurement to reduce length of stay in patients admitted because of preterm labor. Prospective and randomized trial. Final results. Ultrasound in Obstetrics & Gynecology 2006;28(4):485.
References to studies excluded from this review
-
- Beigi A, Zarrinkoub F. Elective versus ultrasound‐indicated cervical cerclage in women at risk for cervical incompetence. Medical Journal of the Islamic Republic of Iran 2005;19(2):103‐7.
-
- Burwick RM, Zork NM, Lee GT, Ross MG, Kjos SL. Cervilenz assessment of cervical length compared to fetal fibronectin in the prediction of preterm delivery in women with threatened preterm labor. Journal of Maternal‐Fetal & Neonatal Medicine 2011;24(1):127‐31. - PubMed
-
- Kassanos D, Salamalekis E, Vitoratos N, Panayotopoulos N, Loghis C, Creatsas C. The value of transvaginal ultrasonography in diagnosis and management of cervical incompetence. Clinical & Experimental Obstetrics & Gynecology 2001;28:266‐8. - PubMed
-
- Lorenz RP, Comstock CH, Bottoms SF, Marx SR. Randomized prospective trial comparing ultrasonography and pelvic examination for preterm labor surveillance. American Journal of Obstetrics and Gynecology 1990;162:1603‐10. - PubMed
-
- Matijevic R, Grgic O, Vasilj O. Is sonographic assessment of cervical length better than digital examination in screening for preterm delivery in a low‐risk population?. Acta Obstetricia et Gynecologica Scandinavica 2006;85(11):1342‐7. - PubMed
Additional references
-
- Berghella V, Bega G, Tolosa JE, Berghella M. Ultrasound assessment of the cervix. Clinical Obstetrics and Gynecology 2003;46:947‐62. - PubMed
-
- Berghella V, Roman A, Daskalakis C, Ness A, Baxter JK. Gestational age at cervical length measurement and incidence of preterm birth. Obstetrics & Gynecology 2007;110:311‐7. - PubMed
-
- Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta‐analysis. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic Reviews in Health Care: Meta‐analysis in Context. London: BMJ Books, 2001.
References to other published versions of this review
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical