

Exercise for improving outcomes after osteoporotic vertebral fracture
- PMID: 23440829
- PMCID: PMC5104540
- DOI: 10.1002/14651858.CD008618.pub2
Exercise for improving outcomes after osteoporotic vertebral fracture
Update in
-
Exercise for improving outcomes after osteoporotic vertebral fracture.Cochrane Database Syst Rev. 2019 Jul 5;7(7):CD008618. doi: 10.1002/14651858.CD008618.pub3. Cochrane Database Syst Rev. 2019. PMID: 31273764 Free PMC article.
Abstract
Background: Vertebral fractures are associated with increased morbidity (e.g., pain, reduced quality of life), and mortality. Therapeutic exercise is a non-pharmacologic conservative treatment that is often recommended for patients with vertebral fractures to reduce pain and restore functional movement.
Objectives: Our objectives were to evaluate the benefits and harms of exercise interventions of four weeks or greater (alone or as part of a physical therapyintervention) versus non-exercise/non-active physical therapy intervention, no intervention or placebo on the incidence of future fractures and adverse events among adults with a history of osteoporotic vertebral fracture(s). We were also examined the effects of exercise on the following secondary outcomes: falls, pain, posture,physical function, balance,mobility, muscle function,quality of life and bone mineral density of the lumbar spine or hip measured using dual-energy X-ray absorptiometry (DXA).We also reported exercise adherence.
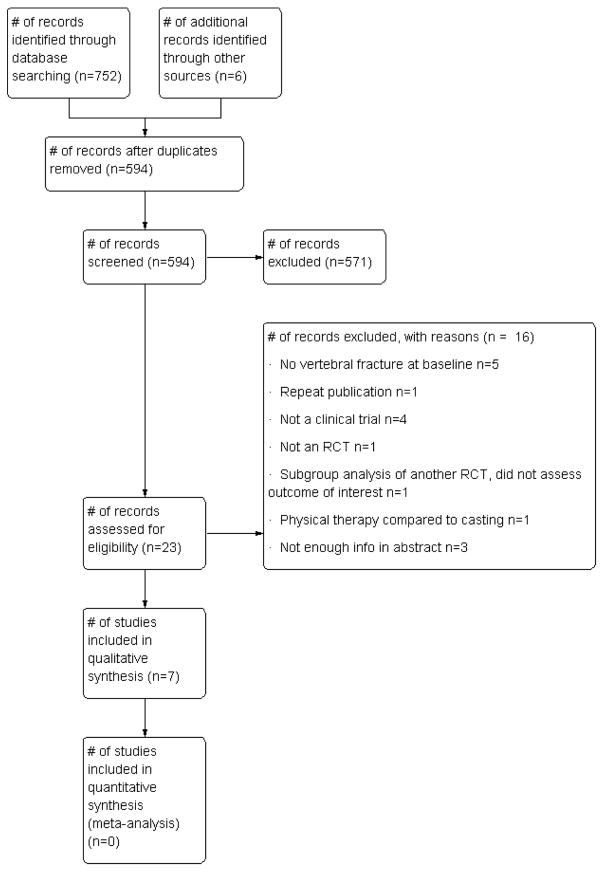
Search methods: We searched the following databases: The Cochrane Library ( Issue 11 of 12, November 2011), MEDLINE (2005 to 2011), EMBASE (1988 to November 23, 2011), CINAHL (Cumulative Index to Nursing and Allied Health Literature, 1982 to November 23, 2011), AMED (1985 to November 2011), and PEDro (Physiotherapy Evidence Database, www.pedro.fhs.usyd.edu.au/index.html, 1929 to November 23, 2011. Ongoing and recently completed trials were identified by searching the World Health Organization International Clinical Trials Registry Platform (to December 2009). Conference proceedings were searched via ISI and SCOPUS, and targeted searches of proceedings of the American Congress of Rehabilitation Medicine and American Society for Bone and Mineral Research. Search terms or MeSH headings included terms such as vertebral fracture AND exercise OR physical therapy.
Selection criteria: We considered all randomized controlled trials and quasi-randomized trials comparing exercise or active physical therapy interventions with placebo/non-exercise/non-active physical therapy interventions or no intervention implemented in individuals with a history of vertebral fracture and evaluating the outcomes of interest.
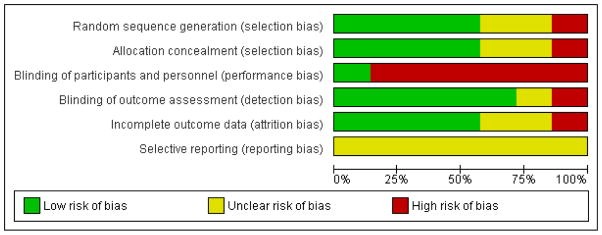
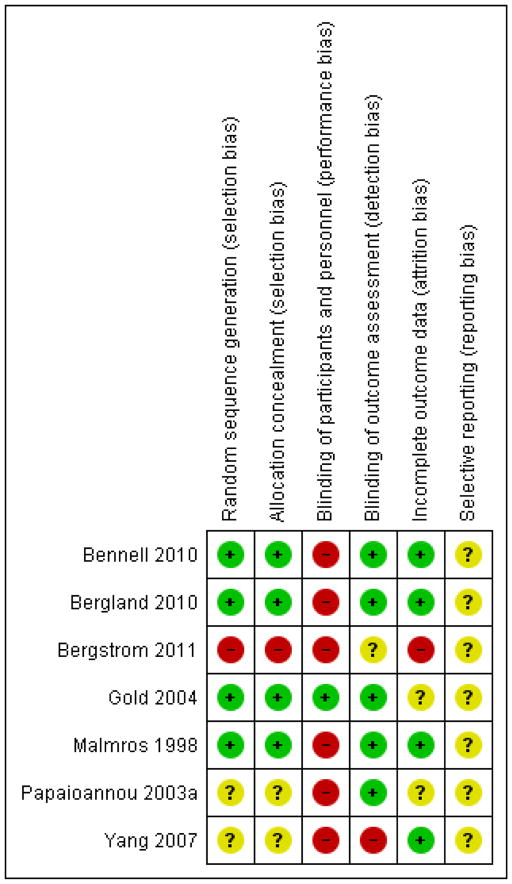
Data collection and analysis: Two review authors independently selected trials and extracted data using a pre-tested data abstraction form. Disagreements were resolved by consensus, or third party adjudication. The Cochrane Collaboration's tool for assessing risk of bias was used to evaluate each study. Studies were grouped according to duration of follow-up (i.e., a) four to 12 weeks; b) 16 to 24 weeks; and c) 52 weeks); a study could be represented in more than one group depending on the number of follow-up assessments. For continuous data, we report mean differences (MDs) of the change or percentage change from baseline. Data from two studies were pooled for one outcome using a fixed-effect model.
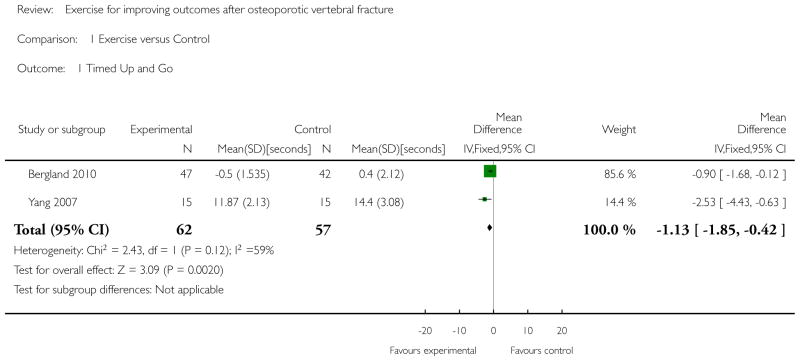
Main results: Seven trials (488 participants, four male participants) were included. Substantial variability across the seven trials prevented any meaningful pooling of data for most outcomes. No trials assessed the effect of exercise on incident fractures, adverse events or incident falls. Individual trials reported that exercise could improve pain, performance on the Timed Up and Go test, walking speed, back extensor strength, trunk muscle endurance, and quality of life. However, the findings should be interpreted with caution given that there were also reports of no significant difference between exercise and control groups for pain, Timed Up and Go test performance, trunk extensor muscle strength and quality of life. Pooled analyses from two studies revealed a significant between-group difference in favour of exercise for Timed Up and Go performance (MD -1.13 seconds, 95% confidence interval (CI) -1.85 to -0.42, P = 0.002). Individual studies also reported no significant between-group differences for posture or bone mineral density. Adherence to exercise varied across studies. The risk of bias across all studies was variable; low risk across most domains in four studies, and unclear or high risk in most domains for three studies.
Authors' conclusions: No definitive conclusions can be made regarding the benefits of exercise for individuals with vertebral fracture. Although individual trials did report benefits for some pain, physical function and quality of life outcomes, the findings should be interpreted with caution given that findings were inconsistent and the quality of evidence was very low. The small number of trials and variability across trials limited our ability to pool outcomes or make conclusions. Evidence regarding the effects of exercise after vertebral fracture, particularly for men, is scarce. A high-quality randomized trial is needed to inform exercise prescription for individuals with vertebral fractures.
Conflict of interest statement
DECLARATIONS OF INTEREST L. Giangregorio: None relevant to this paper. She has received a research grant from Merck Frosst that was awarded in conjunction with an Early Researcher Award from the Ontario Ministry of Research and Innovation. N. MacIntyre: None relevant to this paper. L. Thabane: is a member of an Advisory Board for Network Meta-analysis for GSK. C. Skidmore: None A. Papaioannou: None relevant to this paper. She is or has been a consultant, or on a speaker’s bureau, or received unrestricted grants for the following: Amgen, Eli Lilly, Merck Frosst Canada, Novartis, Pfizer, Warner Chilcott.
Figures
Comment in
-
Exercise prescription for people with osteoporotic vertebral fracture.Br J Sports Med. 2015 Apr;49(7):489-90. doi: 10.1136/bjsports-2013-092652. Epub 2013 Aug 12. Br J Sports Med. 2015. PMID: 23940270 No abstract available.
References
References to studies included in this review
-
- Bennell KL, Matthews B, Greig A, Briggs A, Kelly A, Sherburn M, et al. Effects of an exercise and manual therapy program on physical impairments, function and quality-of-life in people with osteoporotic vertebral fracture: a randomised, single-blind controlled pilot trial. BMC Musculoskelet Disord. 2010;11:36. - PMC - PubMed
-
- Bergland A, Thorsen H, Karesen R. Effect of exercise on mobility, balance, and health-related quality of life in osteoporotic women with a history of vertebral fracture: a randomized, controlled trial. Osteoporosis International. 2011;22(6):1863–71. - PubMed
-
- Bergstrom I, Bergstrom K, Kronhed A, Karlsson S, Brinck J. Back extensor training increases muscle strength in postmenopausal women with osteoporosis, kyphosis and vertebral fractures. Advances in Physiotherapy. 2011;13(3):110–7.
-
- Gold DT, Shipp KM, Pieper CF, Duncan PW, Martinez S, Lyles KW. Group treatment improves trunk strength and psychological status in older women with vertebral fractures: results of a randomized, clinical trial. Journal of the American Geriatrics Society. 2004;52(9):1471–8. - PubMed
-
- Malmros B, Mortensen L, Jensen MB, Charles P. Positive effects of physiotherapy on chronic pain and performance in osteoporosis. Osteoporos Int. 1998;8(3):215–21. - PubMed
References to studies excluded from this review
-
- Bada AM, Rodriguez JE. What are the best treatments for reducing pain due to compression fractures? Evidence Based Practice. 2009;12(1):4–5.
-
- Bautmans I, Van Arken J, Van Mackelenberg M, Mets T. Rehabilitation using manual mobilization for thoracic kyphosis in elderly postmenopausal patients with osteoporosis. Journal of Rehabilitation Medicine. 2010;42:129–35. - PubMed
-
- Borgo MJ, Sinaki M. Back progressive resistive exercise program to reduce risk of vertebral fractures. Journal für Mineralstoffwechsel. 2010;17(2):66–71.
-
- Hongo M, Itoi E, Sinaki M, Miyakoshi N, Shimada Y, Maekawa S, et al. Effect of low-intensity back exercise on quality of life and back extensor strength in patients with osteoporosis: a randomized controlled trial. Osteoporosis International. 2007;18(10):1389–95. - PubMed
-
- Lord SR, Ward JA, Williams P, Zivanovic E. The effects of a community exercise program on fracture risk factors in older women. Osteoporosis International. 1996;6(5):361–7. - PubMed
Additional references
-
- Adachi JD, Loannidis G, Berger C, Joseph L, Papaioannou A, Pickard L, et al. The influence of osteoporotic fractures on health-related quality of life in community-dwelling men and women across Canada. Osteoporosis International. 2001;12(11):903–8. - PubMed
-
- Bennell K, Khan K, McKay H. The role of physiotherapy in the prevention and treatment of osteoporosis. Manual Therapy. 2000;5(4):198–213. - PubMed
-
- Bessette L, Ste-Marie LG, Jean S, Davison KS, Beaulieu M, Baranci M, et al. Recognizing osteoporosis and its consequences in Quebec (ROCQ); background, rationale and methods of an anti-fracture patient health-management programme. Contemporary Clinical Trials. 2008;29(2):194–210. - PubMed
-
- Briggs AM, van Dieën JH, Wrigley TV, Greig AM, Phillips B, Lo SK, et al. Thoracic kyphosis affects spinal loads and trunk muscle force. Physical Therapy. 2007;87(5):595–607. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous