

Is lymphatic status related to regression of inflammation in Crohn's disease?
- PMID: 23443404
- PMCID: PMC3582160
- DOI: 10.4240/wjgs.v4.i10.228
Is lymphatic status related to regression of inflammation in Crohn's disease?
Abstract
Aim: To investigate the status of the lymphatic vessels in the small bowel affected by Crohn's disease (CD) at the moment of surgery.
Methods: During the period January 2011-June 2011, 25 consecutive patients affected by CD were operated on in our Institution. During surgery, Patent Blue V was injected subserosally and the way it spread along the subserosa of the intestinal wall, through the mesenterial layers towards the main lymphatic collectors and eventually to the lymph nodes was observed and recorded. Since some patients had been undergone strictureplasty at previous surgery, we also examined the status of intestinal lymph vessels after previous strictureplasties. The same procedure was performed in a control group of 5 patients affected by colorectal cancer. Length of lesions, caliber, maximal thickness of the diseased intestinal wall, thickness of the wall at injection site and thickness of the mesentery were evaluated at surgery.
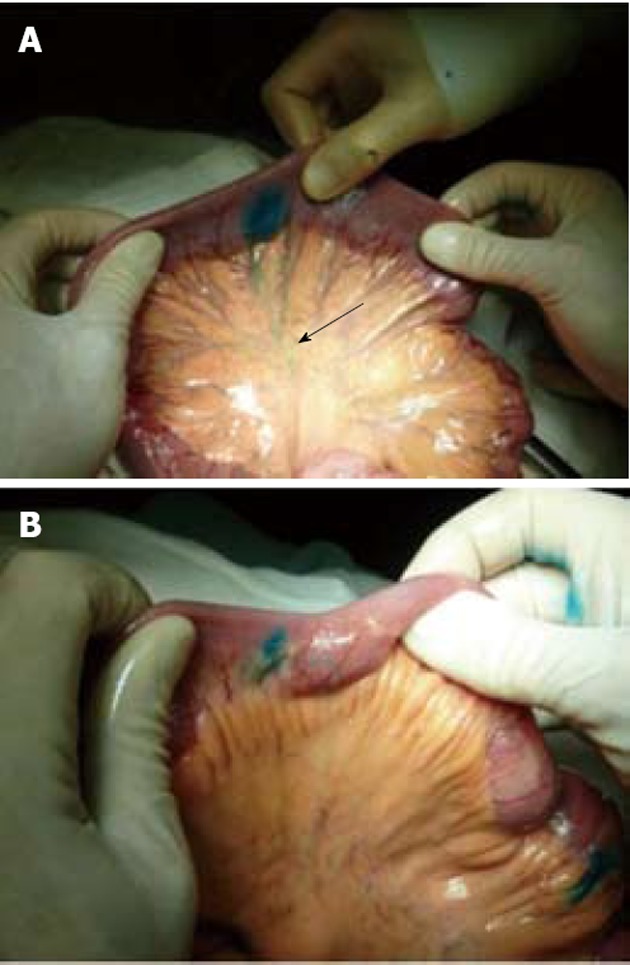
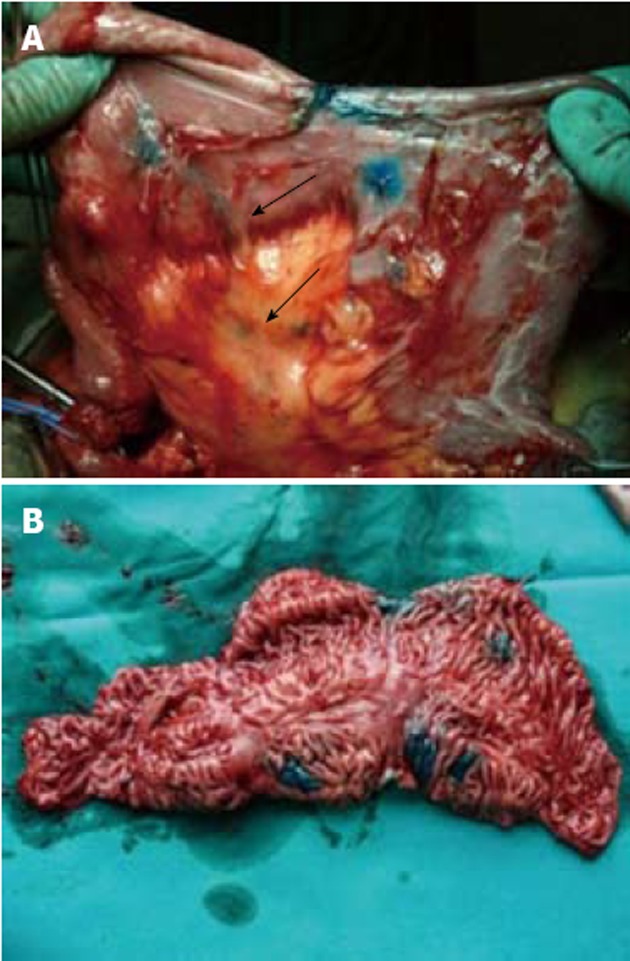
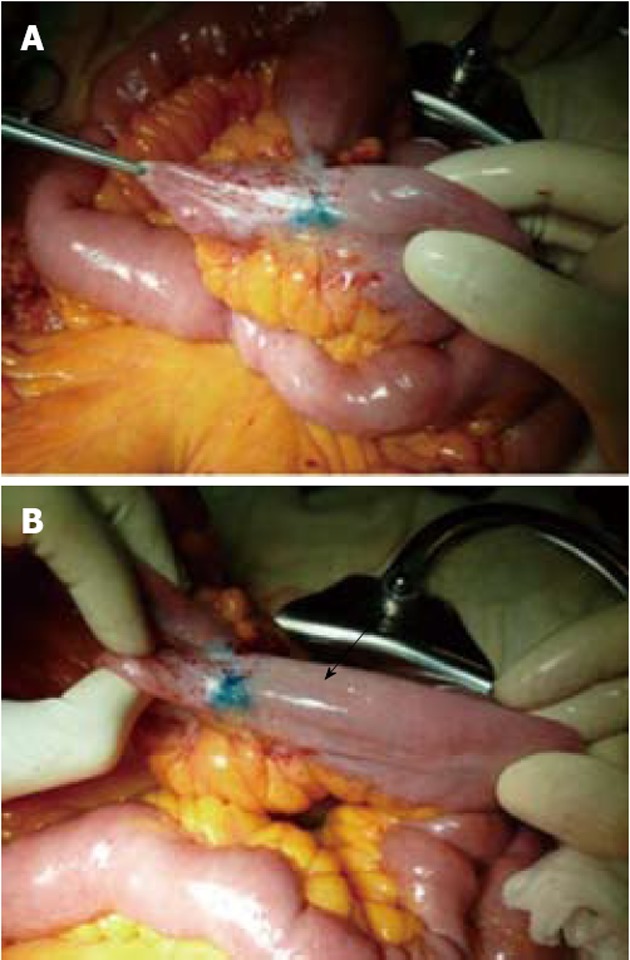
Results: We observed three features after the injection of Patent Blue V in the intestinal loops: (1) Macroscopically healthy terminal ileum of patients with CD or colon cancer showed thin lymphatic vessels linearly directed toward the mesentery; (2) In mild lesions in which the intestinal wall did not reach 8 mm of thickness, we observed short, wide and tortuous lymphatic vessels directed longitudinally along the intestinal axis toward disease-free areas and then transversally toward the mesentery; and (3) Injection in the severely affected lesions, that had a thickness of the intestinal wall over 10 mm, did not show any feature of lymphatic vessels at least on the subserosal surface. There was a correlation between the thickness of the parietal wall and the severity of the lymphatic alterations. Normal lymphatic vessels were observed at previous strictureplasties in the presence of complete regression of the inflammation.
Conclusion: Injection of Patent Blue V in the intestinal wall could help distinguish healthy tracts of the small bowel from those macroscopically borderline.
Keywords: Crohn’s disease; Inlflammation; Intestinal wall; Lymphatic vessels; Mesentery; Patent blue V; Strictureplasty; Surgery; Thickness.
Figures


References
-
- Van Kruiningen HJ, Colombel JF. The forgotten role of lymphangitis in Crohn’s disease. Gut. 2008;57:1–4. - PubMed
-
- Blackburn G, Hadfield G, Hunt AH. Regional ileitis. St Bart's Hosp Rep. 1939;72:181–224.
-
- Van Patter WN. Pathology and pathogenesis of regional enteritis (Dissertation). Minneapolis, Minn. University of Minnesota; 1952.
-
- Kalima TV. Experimental lymphatic obstruction in the ileum. Ann Chir Gynaecol Fenn. 1970;59:187–201. - PubMed
LinkOut - more resources
Full Text Sources
