

Combining cognitive-behavioral therapy and milnacipran for fibromyalgia: a feasibility randomized-controlled trial
- PMID: 23446065
- PMCID: PMC4185390
- DOI: 10.1097/AJP.0b013e31827a784e
Combining cognitive-behavioral therapy and milnacipran for fibromyalgia: a feasibility randomized-controlled trial
Abstract
Objectives: To evaluate the feasibility of a randomized-controlled trial and to obtain estimates of the effects of combined cognitive-behavioral therapy (CBT) and milnacipran for the treatment of fibromyalgia.
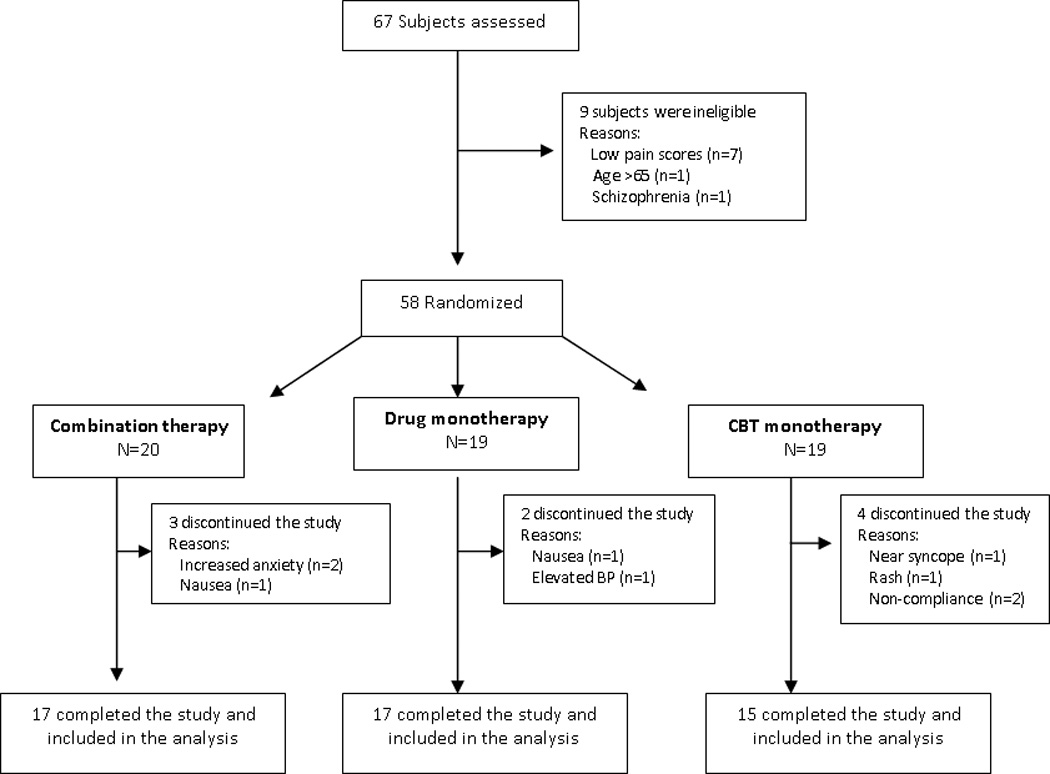
Methods: Fifty-eight patients with fibromyalgia were randomized to 1 of the 3 treatment arms: (1) combination therapy (n = 20); (2) milnacipran+education (n = 19); and (3) placebo+CBT (n = 19). Patients received either milnacipran (100 mg/d) or placebo. Patients also received 8 sessions of phone-delivered CBT or educational instructions, but only from baseline to week 9. Assessments were conducted at baseline, week 9, and 21. The primary endpoints were baseline to week 21 changes in weekly average pain intensity and physical function (SF-36 physical function scale).
Results: Compared with milnacipran, combination therapy demonstrated a moderate effect on improving SF-36 physical function (SE = 9.42 [5.48], P = 0.09, effect size = 0.60) and in reducing weekly average pain intensity (mean difference [SE] = -1.18 [0.62], P = 0.07, effect size = 0.67). Compared with milnacipran, CBT had a moderate to large effect in improving SF-36 physical function (mean difference [SE] = 11.0 [5.66], P = 0.06, effect size = 0.70). Despite the presence of concomitant centrally acting therapies, dropout rate was lower than anticipated (15% at week 21). Importantly, at least 6 out of the 8 phone-based therapy sessions were successfully completed by 89% of the patients; and adherence to the treatment protocols was > 95%.
Conclusions: In this pilot study, a therapeutic approach that combines phone-based CBT and milnacipran was feasible and acceptable. Moreover, the preliminary data supports conducting a fully powered randomized-controlled trial.
Trial registration: ClinicalTrials.gov NCT01038323.
Conflict of interest statement
No conflicts of interest to declare
References
-
- Wolfe F, Ross K, Anderson J, Russell IJ, Hebert L. The prevalence and characteristics of fibromyalgia in the general population. Arthritis Rheum. 1995;38(1):19–28. - PubMed
-
- Hauser W, Bernardy K, Uceyler N, Sommer C. Treatment of fibromyalgia syndrome with antidepressants: a meta-analysis. JAMA. 2009;301(2):198–209. - PubMed
-
- Hauser W, Bernardy K, Uceyler N, Sommer C. Treatment of fibromyalgia syndrome with gabapentin and pregabalin--a meta-analysis of randomized controlled trials. Pain. 2009;145(1–2):69–81. - PubMed
-
- Hassett AL, Williams DA. Non-pharmacological treatment of chronic widespread musculoskeletal pain. Best Pract Res Clin Rheumatol. 2011;25(2):299–309. - PubMed
-
- Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33(2):160–172. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
