

Emergency department services use among immigrant and non-immigrant groups in the United States
- PMID: 23447058
- PMCID: PMC3779496
- DOI: 10.1007/s10903-013-9802-z
Emergency department services use among immigrant and non-immigrant groups in the United States
Abstract
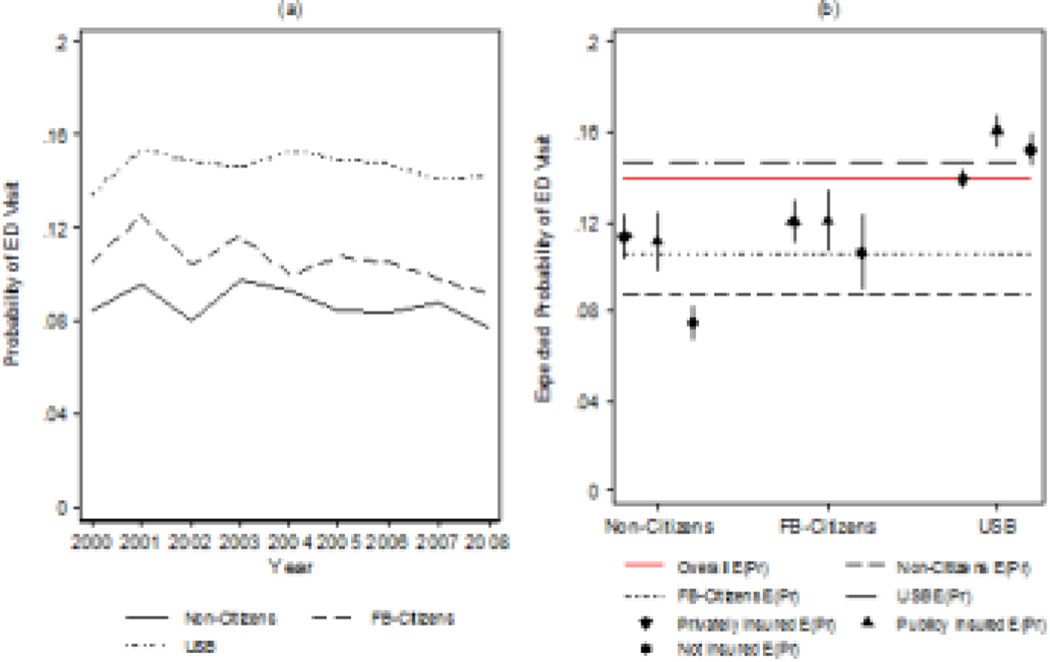
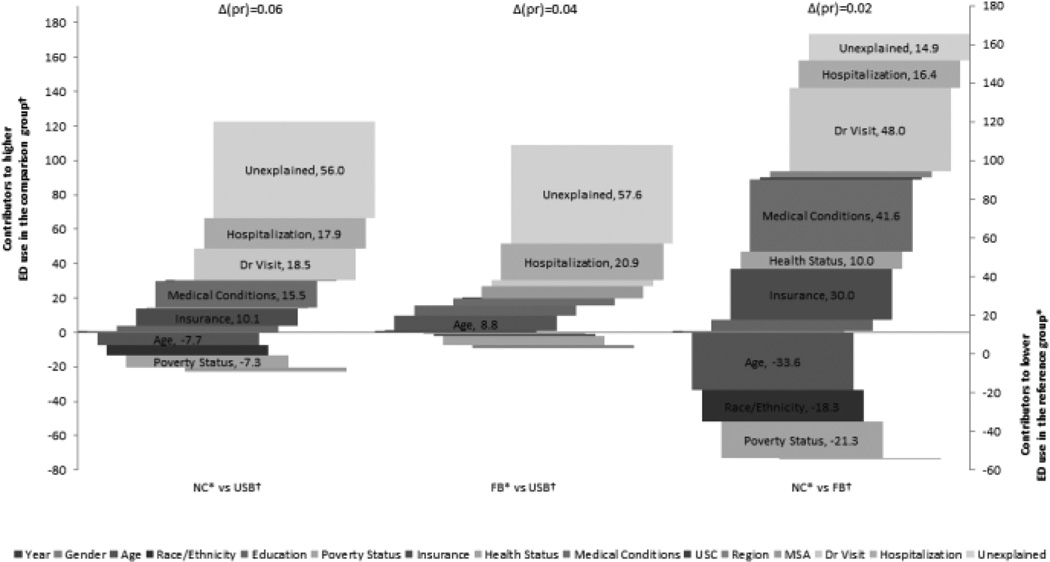
Immigrants have disproportionate lack of access to healthcare and insurance. Emergency departments could serve as a healthcare substitute and increased demand can negatively affect the US emergency services system. Medical Expenditures Panel Survey (2000-2008) data was modeled to compare emergency departments (ED) use between non-citizens, foreign-born (naturalized), and US-born citizens. Group differences were assessed using non-linear decomposition techniques. Non-citizens were less likely to use ED services (8.7 %) compared to naturalized immigrants (10.6 %) and US-born Americans (14.7 %). Differences in ED use persisted after adjusting for the Behavioral Model covariates. Healthcare need and insurance partially explained the differences in ED use between the groups. Between 2000 and 2008 non-citizen immigrants used markedly less ED services compared to US citizens, regardless of their nation of origin. We also found that demographic and healthcare need profiles contributed to the divergence in use patterns between groups. A less restrictive healthcare policy environment can potentially contribute to lower population disease burden and greater efficiencies in the US health care system.
Conflict of interest statement
Figures
References
-
- Passel JS, Cohn DV. U.S. Population Projections: 2005–2050. Washington, DC: Pew Research Center; 2008. Accessed from http://pewhispanic.org/files/reports/85.pdf on February, 17th 2011.
-
- Kandula NR, Kersey M, Lurie N. Assuring the Health of Immigrants: What the Leading Health Indicators Tell Us. Annual Review of Public Health. 2004;25(1):357–376. - PubMed
-
- Derose KP, Bahney BW, Lurie N, Escarce JJ. Immigrants and Health Care Access, Quality, and Cost. Medical Care Research and Review. 2009 - PubMed
-
- Derose KP, Escarce JJ, Lurie N. Immigrants And Health Care: Sources Of Vulnerability. Health Affairs. 2007 Sep 1;26(5):1258–1268. 2007. - PubMed
-
- Lee S, Choi S. Disparities in access to health care among non-citizens in the United States. Health Sociology Review. 2009;18(3):307–314.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
