

The effect of statins on testosterone in men and women, a systematic review and meta-analysis of randomized controlled trials
- PMID: 23448151
- PMCID: PMC3621815
- DOI: 10.1186/1741-7015-11-57
The effect of statins on testosterone in men and women, a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Statins are extensively used for cardiovascular disease prevention. Statins reduce mortality rates more than other lipid-modulating drugs, although evidence from randomized controlled trials also suggests that statins unexpectedly increase the risk of diabetes and improve immune function. Physiologically, statins would be expected to lower androgens because statins inhibit production of the substrate for the local synthesis of androgens and statins' pleiotropic effects are somewhat similar to the physiological effects of lowering testosterone, so we hypothesized that statins lower testosterone.
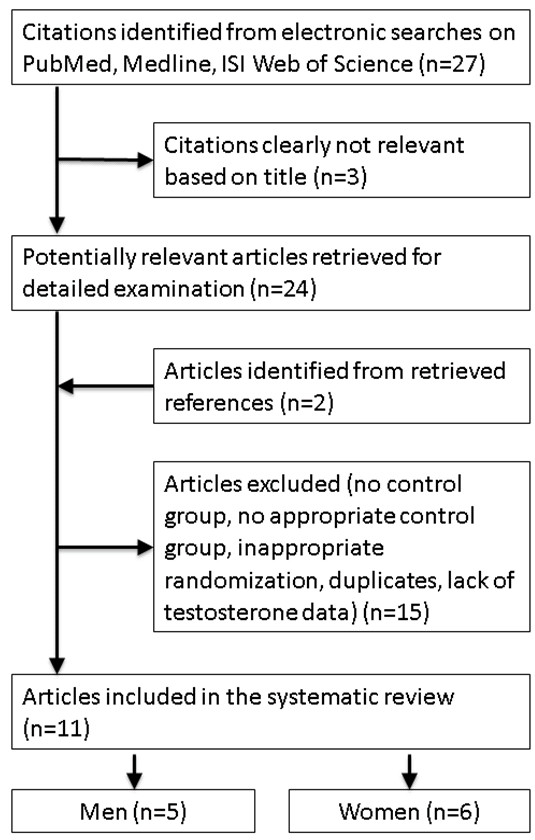
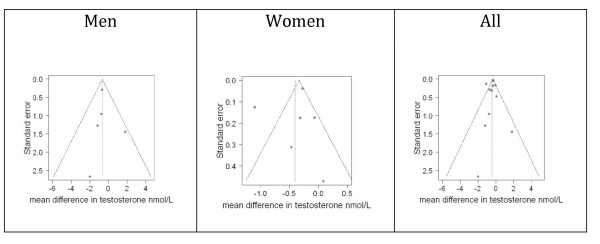
Methods: A meta-analysis of placebo-controlled randomized trials of statins to test the a priori hypothesis that statins lower testosterone. We searched the PubMed, Medline and ISI Web of Science databases until the end of 2011, using '(Testosterone OR androgen) AND (CS-514 OR statin OR simvastatin OR atorvastatin OR fluvastatin OR lovastatin OR rosuvastatin OR pravastatin)' restricted to randomized controlled trials in English, supplemented by a bibliographic search. We included studies with durations of 2+ weeks reporting changes in testosterone. Two reviewers independently searched, selected and assessed study quality. Two statisticians independently abstracted and analyzed data, using random or fixed effects models, as appropriate, with inverse variance weighting.
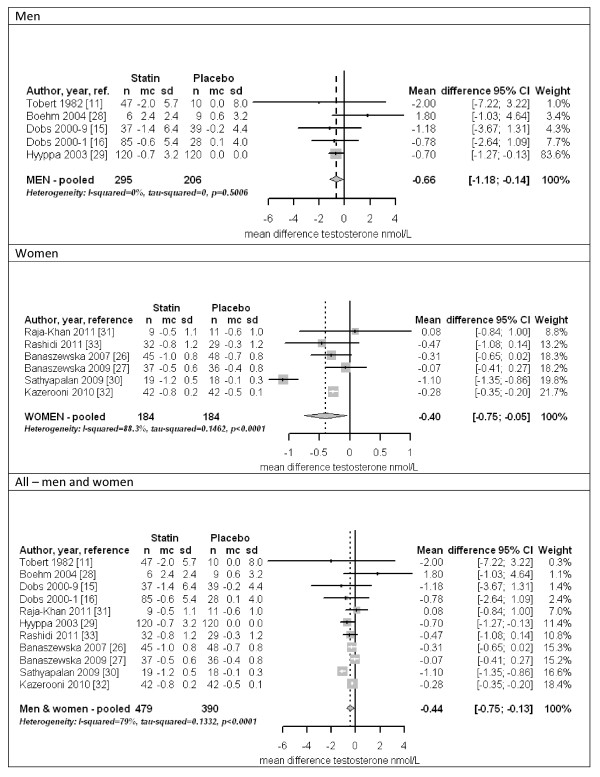
Results: Of the 29 studies identified 11 were eligible. In 5 homogenous trials of 501 men, mainly middle aged with hypercholesterolemia, statins lowered testosterone by -0.66 nmol/l (95% confidence interval (CI) -0.14 to -1.18). In 6 heterogeneous trials of 368 young women with polycystic ovary syndrome, statins lowered testosterone by -0.40 nmol/l (95% CI -0.05 to -0.75). Overall statins lowered testosterone by -0.44 nmol/l (95% CI -0.75 to -0.13).
Conclusions: Statins may partially operate by lowering testosterone. Whether this is a detrimental side effect or mode of action warrants investigation given the potential implications for drug development and prevention of non-communicable chronic diseases. See commentary article here http://www.biomedcentral.com/1741-7015/11/58.
Figures
Comment in
-
Do statins lower testosterone and does it matter?BMC Med. 2013 Feb 28;11:58. doi: 10.1186/1741-7015-11-58. BMC Med. 2013. PMID: 23448188 Free PMC article.
References
-
- Sattar N, Preiss D, Murray HM, Welsh P, Buckley BM, de Craen AJ, Seshasai SR, McMurray JJ, Freeman DJ, Jukema JW, Macfarlane PW, Packard CJ, Stott DJ, Westendorp RG, Shepherd J, Davis BR, Pressel SL, Marchioli R, Marfisi RM, Maggioni AP, Tavazzi L, Tognoni G, Kjekshus J, Pedersen TR, Cook TJ, Gotto AM, Clearfield MB, Downs JR, Nakamura H, Ohashi Y. et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet. 2010;375:735–742. doi: 10.1016/S0140-6736(09)61965-6. - DOI - PubMed
-
- Preiss D, Seshasai SR, Welsh P, Murphy SA, Ho JE, Waters DD, DeMicco DA, Barter P, Cannon CP, Sabatine MS, Braunwald E, Kastelein JJ, de Lemos JA, Blazing MA, Pedersen TR, Tikkanen MJ, Sattar N, Ray KK. Risk of incident diabetes with intensive-dose compared with moderate-dose statin therapy: a meta-analysis. JAMA. 2011;305:2556–2564. doi: 10.1001/jama.2011.860. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
