

Prevalence dependent calibration of a predictive model for nasal carriage of methicillin-resistant Staphylococcus aureus
- PMID: 23448529
- PMCID: PMC3599956
- DOI: 10.1186/1471-2334-13-111
Prevalence dependent calibration of a predictive model for nasal carriage of methicillin-resistant Staphylococcus aureus
Abstract
Background: Published models predicting nasal colonization with Methicillin-resistant Staphylococcus aureus among hospital admissions predominantly focus on separation of carriers from non-carriers and are frequently evaluated using measures of discrimination. In contrast, accurate estimation of carriage probability, which may inform decisions regarding treatment and infection control, is rarely assessed. Furthermore, no published models adjust for MRSA prevalence.
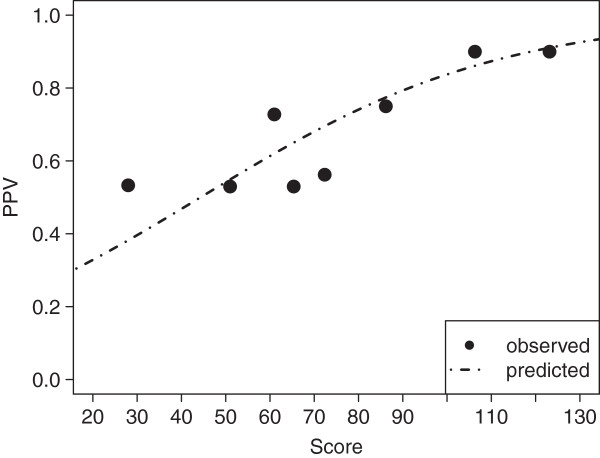
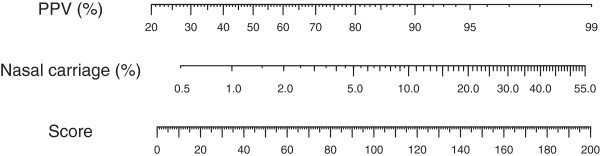
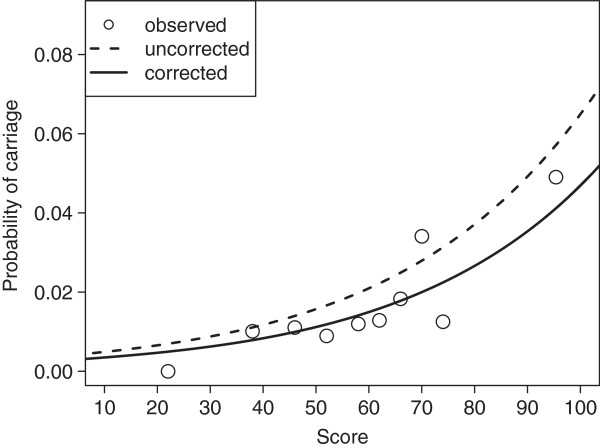
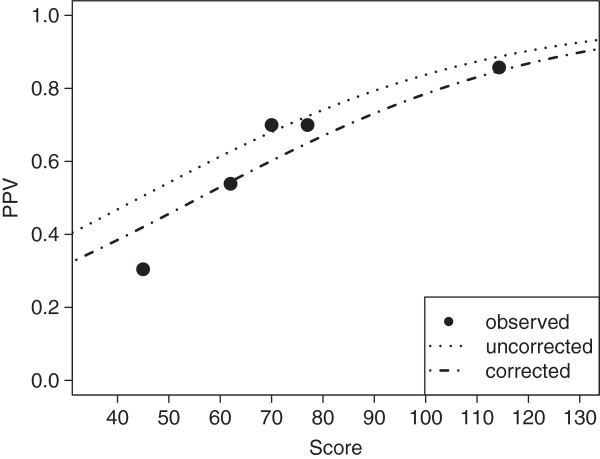
Methods: Using logistic regression, a scoring system (values from 0 to 200) predicting nasal carriage of MRSA was created using a derivation cohort of 3091 individuals admitted to a European tertiary referral center between July 2007 and March 2008. The expected positive predictive value of a rapid diagnostic test (GeneOhm, Becton & Dickinson Co.) was modeled using non-linear regression according to score. Models were validated on a second cohort from the same hospital consisting of 2043 patients admitted between August 2008 and January 2012. Our suggested correction score for prevalence was proportional to the log-transformed odds ratio between cohorts. Calibration before and after correction, i.e. accurate classification into arbitrary strata, was assessed with the Hosmer-Lemeshow-Test.
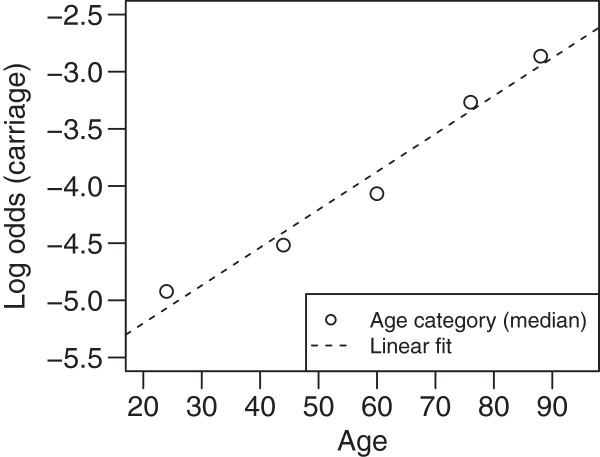
Results: Treating culture as reference, the rapid diagnostic test had positive predictive values of 64.8% and 54.0% in derivation and internal validation corhorts with prevalences of 2.3% and 1.7%, respectively. In addition to low prevalence, low positive predictive values were due to high proportion (> 66%) of mecA-negative Staphylococcus aureus among false positive results. Age, nursing home residence, admission through the medical emergency department, and ICD-10-GM admission diagnoses starting with "A" or "J" were associated with MRSA carriage and were thus included in the scoring system, which showed good calibration in predicting probability of carriage and the rapid diagnostic test's expected positive predictive value. Calibration for both probability of carriage and expected positive predictive value in the internal validation cohort was improved by applying the correction score.
Conclusions: Given a set of patient parameters, the presented models accurately predict a) probability of nasal carriage of MRSA and b) a rapid diagnostic test's expected positive predictive value. While the former can inform decisions regarding empiric antibiotic treatment and infection control, the latter can influence choice of screening method.
Figures


References
-
- Köck R, Becker K, Cookson B, Van Gemert-Pijnen JE, Harbarth S, Kluytmans J, Mielke M, Peters G, Skov RL, Struelens MJ, Tacconelli E, Navarro Torné A, Witte W, Friedrich AW. Methicillin-resistant Staphylococcus aureus (MRSA): burden of disease and control challenges in Europe. Euro Surveill. 2010;15:19688. - PubMed
-
- Klevens RM, Morrison MA, Nadle J, Petit S, Gershman K, Ray S, Harrison LH, Lynfield R, Dumyati G, Townes JM, Craig AS, Zell ER, Fosheim GE, McDougal LK, Carey RB, Fridkin SK. For the Active Bacterial Core surveillance (ABCs) MRSA Investigators. Invasive methicillin-resistant staphylococcus aureus infections in the United States. JAMA. 2007;298:1763–1771. doi: 10.1001/jama.298.15.1763. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
