

Cord lining-mesenchymal stem cells graft supplemented with an omental flap induces myocardial revascularization and ameliorates cardiac dysfunction in a rat model of chronic ischemic heart failure
- PMID: 23448654
- PMCID: PMC3638562
- DOI: 10.1089/ten.tea.2012.0407
Cord lining-mesenchymal stem cells graft supplemented with an omental flap induces myocardial revascularization and ameliorates cardiac dysfunction in a rat model of chronic ischemic heart failure
Abstract
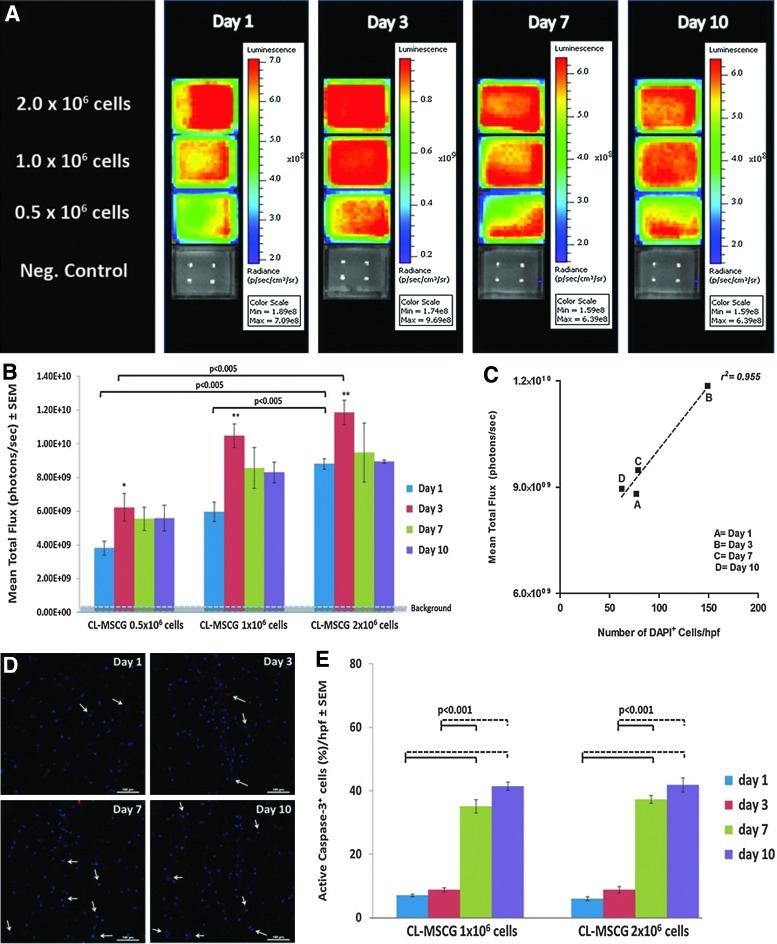
Myocardial restoration using tissue-engineered grafts to regenerate the ischemic myocardium offers improved donor cell retention, yet a limited cell survival resulting from poor vascularization needs to be addressed. A cell type derived from the subamnion, namely, cord-lining mesenchymal stem cells (CL-MSC), has recently been identified. Here we present a restorative strategy that combines a fibrin graft containing human CL-MSC and omental flap providing, thereby, cell-, structural-, and angiogenic support to the injured myocardium. The graft consisted of a mixture of 2×10(6) CL-MSC-GFP-Fluc and fibrin. Myocardial infarction (MI) was induced in nude rats and following confirmation of ensued heart failure with echocardiography 2 weeks after injury, therapeutic intervention was performed as follows: untreated (MI, n=7), CL-MSC graft (CL-MSCG, n=8), CL-MSCG and omental flap (CL-MSCG+OM, n=11), and omental flap (OM, n=8). In vivo bioluminescence imaging at 1, 3, 7, and 14 days post-treatment indicated comparable early donor cell viability between the CL-MSCG and CL-MSCG+OM. Treatment with CL-MSCG+OM improved the myocardial function as assessed by the measurement of end-diastolic left ventricular (LV) pressure (3.53±0.34 vs. 5.21±0.54 mmHg, p<0.05), contractility (+dP/dt, 3383.8±250.78 mmHg vs. 2464.9±191.8 mmHg, p<0.05), and the relaxation rate (-dP/dt, -2707.2±250.7 mmHg vs. 1948.7±207.8 mmHg, p<0.05), compared to MI control 6 weeks after ischemic injury. Furthermore, evidence of a 20.32% increase in the ejection fraction was observed in CL-MSCG+OM rats from week 2 to 6 after injury. Both CL-MSCG and CL-MSCG+OM led to an enhanced cardiac output (p<0.05), and attenuated the infarct size (35.7%±4.2% and 34.7%±4.8%), as compared to MI (60.7%±3.1%; p<0.01 and p<0.001, respectively). All treated groups had a higher arteriole density than controls. Yet, a higher amount of functional blood vessels, and a 20-fold increase in arteriole numbers were found in CL-MSCG+OM. Altogether, CL-MSCGs supplemented with vascular supply have the potential to repair the failing, chronically ischemic heart by improving myocardial revascularization, attenuating remodeling, and ameliorating cardiac dysfunction.
Figures




Similar articles
-
Grafts enriched with subamnion-cord-lining mesenchymal stem cell angiogenic spheroids induce post-ischemic myocardial revascularization and preserve cardiac function in failing rat hearts.Stem Cells Dev. 2013 Dec 1;22(23):3087-99. doi: 10.1089/scd.2013.0119. Epub 2013 Aug 31. Stem Cells Dev. 2013. PMID: 23869939 Free PMC article.
-
Post-ischaemic angiogenic therapy using in vivo prevascularized ascorbic acid-enriched myocardial artificial grafts improves heart function in a rat model.J Tissue Eng Regen Med. 2013 Mar;7(3):203-12. doi: 10.1002/term.512. Epub 2011 Oct 28. J Tissue Eng Regen Med. 2013. PMID: 22034461
-
Human Umbilical Cord-Derived Mesenchymal Stromal Cells Improve Left Ventricular Function, Perfusion, and Remodeling in a Porcine Model of Chronic Myocardial Ischemia.Stem Cells Transl Med. 2016 Aug;5(8):1004-13. doi: 10.5966/sctm.2015-0298. Epub 2016 Jun 22. Stem Cells Transl Med. 2016. PMID: 27334487 Free PMC article.
-
Clinical aspects of left ventricular diastolic function assessed by Doppler echocardiography following acute myocardial infarction.Dan Med Bull. 2001 Nov;48(4):199-210. Dan Med Bull. 2001. PMID: 11767125 Review.
-
Application of mesenchymal stem cell sheet to treatment of ischemic heart disease.Stem Cell Res Ther. 2021 Jul 7;12(1):384. doi: 10.1186/s13287-021-02451-1. Stem Cell Res Ther. 2021. PMID: 34233729 Free PMC article. Review.
Cited by
-
Grafts enriched with subamnion-cord-lining mesenchymal stem cell angiogenic spheroids induce post-ischemic myocardial revascularization and preserve cardiac function in failing rat hearts.Stem Cells Dev. 2013 Dec 1;22(23):3087-99. doi: 10.1089/scd.2013.0119. Epub 2013 Aug 31. Stem Cells Dev. 2013. PMID: 23869939 Free PMC article.
-
Cell-Based Therapies for Cardiac Regeneration: A Comprehensive Review of Past and Ongoing Strategies.Int J Mol Sci. 2018 Oct 16;19(10):3194. doi: 10.3390/ijms19103194. Int J Mol Sci. 2018. PMID: 30332812 Free PMC article. Review.
-
Current indications for the intrathoracic transposition of the omentum.J Cardiothorac Surg. 2019 Jun 10;14(1):103. doi: 10.1186/s13019-019-0924-9. J Cardiothorac Surg. 2019. PMID: 31182112 Free PMC article. Review.
-
Cord Lining Mesenchymal Stem Cells Have a Modest Positive Effect on Angiogenesis in Hindlimb Ischemia.Front Cell Dev Biol. 2021 Mar 8;8:596170. doi: 10.3389/fcell.2020.596170. eCollection 2020. Front Cell Dev Biol. 2021. PMID: 33763413 Free PMC article.
-
Enhanced Immunomodulation in Inflammatory Environments Favors Human Cardiac Mesenchymal Stromal-Like Cells for Allogeneic Cell Therapies.Front Immunol. 2019 Jul 23;10:1716. doi: 10.3389/fimmu.2019.01716. eCollection 2019. Front Immunol. 2019. PMID: 31396228 Free PMC article.
References
-
- Lloyd-Jones D. Adams R.J. Brown T.M. Carnethon M. Dai S. De Simone G. Ferguson T.B. Ford E. Furie K. Gillespie C. Go A. Greenlund K. Haase N. Hailpern S. Ho P.M. Howard V. Kissela B. Kittner S. Lackland D. Lisabeth L. Marelli A. McDermott M.M. Meigs J. Mozaffarian D. Mussolino M. Nichol G. Roger V.L. Rosamond W. Sacco R. Sorlie P. Stafford R. Thom T. Wasserthiel-Smoller S. Wong N.D. Wylie-Rosett J. Executive summary: heart disease and stroke statistics—2010 update: a report from the American Heart Association. Circulation. 2010;121:948. - PubMed
-
- Martinez E.C. Kofidis T. Adult stem cells for cardiac tissue engineering. J Mol Cell Cardiol. 2011;50:312. - PubMed
-
- Kinnaird T. Stabile E. Burnett M.S. Lee C.W. Barr S. Fuchs S. Epstein S.E. Marrow-derived stromal cells express genes encoding a broad spectrum of arteriogenic cytokines and promote in vitro and in vivo arteriogenesis through paracrine mechanisms. Circ Res. 2004;94:678. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
