

Response to CPAP withdrawal in patients with mild versus severe obstructive sleep apnea/hypopnea syndrome
- PMID: 23449493
- PMCID: PMC3571747
- DOI: 10.5665/sleep.2460
Response to CPAP withdrawal in patients with mild versus severe obstructive sleep apnea/hypopnea syndrome
Abstract
Background: Patients with obstructive sleep apnea/hypopnea syndrome (OSAHS), even those generally compliant with CPAP therapy, often intermittently discontinue CPAP.
Study objective: Examine the impact of CPAP withdrawal on sleep, sleep disordered breathing (SDB), and daytime function in subjects with varying severity of OSAHS.
Patients and interventions: Forty-two subjects (26M/16 F) with OSAHS (AHI4% = 45.2 ± 35.5/h pretreatment) on CPAP for 4 months were evaluated on the second night of CPAP withdrawal. Sleep architecture, SDB indices, and subjective/objective daytime function were assessed pretreatment, on CPAP therapy, and after CPAP withdrawal. Comparisons were made between pretreatment and CPAP withdrawal for the entire group, and for subgroups of mild/moderate (AHI4% < 30/h, n = 22) and severe (AHI4% > 30/h, n = 20) SDB.
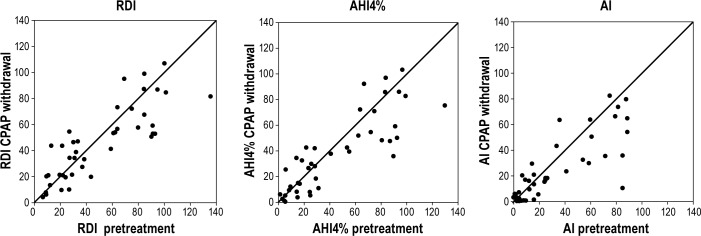
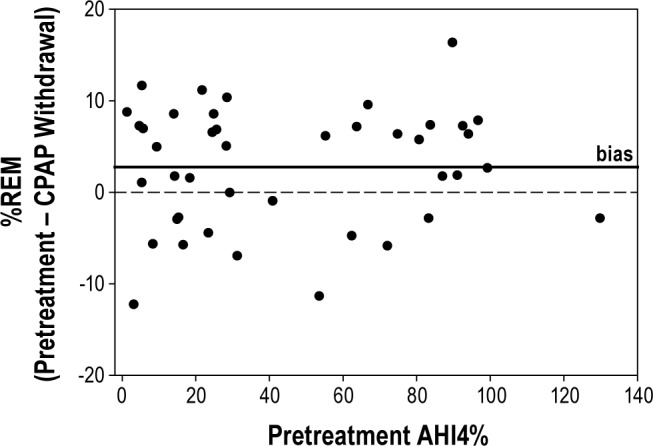
Results: Overall, and for mild/moderate subjects, SDB indices returned to pretreatment values on CPAP withdrawal but with fewer apneas and more hypopneas/RERAs. For severe SDB, the event frequency (AI, AHI4%, and RDI) was lower and O2 desaturation was improved on CPAP withdrawal. Across SDB severity, sleep architecture showed lower %REM (15.6% vs 12.9%, P = 0.009) on the CPAP withdrawal compared to pretreatment. Stanford Sleepiness Score, MSLT, and PVT measures were not significantly different between pretreatment and CPAP withdrawal.
Conclusions: Over a wide range of SDB severity CPAP withdrawal results in recurrence of SDB, albeit with less severe O2 desaturation. Subjective/objective daytime function returned to pretreatment levels. Sleep architecture changes on CPAP withdrawal (acute SDB) may reflect reduced sleep pressure compared to pretreatment chronic SDB. Our data suggest detrimental effects of even brief withdrawal of CPAP in subjects with both mild and severe OSAHS.
Citation: Young LR; Taxin ZH; Norman RG; Walsleben JA; Rapoport DM; Ayappa I. Response to CPAP withdrawal in patients with mild versus severe obstructive sleep apnea/hypopnea syndrome. SLEEP 2013;36(3):405-412.
Keywords: CPAP withdrawal; daytime sleepiness; sleep disordered breathing.
Figures

Similar articles
-
Multinight recording and analysis of continuous positive airway pressure airflow in the home for titration and management of sleep disordered breathing.Sleep. 2013 Apr 1;36(4):535-545F. doi: 10.5665/sleep.2540. Sleep. 2013. PMID: 23543909 Free PMC article.
-
Randomized controlled trial of variable-pressure versus fixed-pressure continuous positive airway pressure (CPAP) treatment for patients with obstructive sleep apnea/hypopnea syndrome (OSAHS).Sleep. 2010 Feb;33(2):267-71. doi: 10.1093/sleep/33.2.267. Sleep. 2010. PMID: 20175411 Free PMC article. Clinical Trial.
-
Sleep quality, short-term and long-term CPAP adherence.J Clin Sleep Med. 2012 Oct 15;8(5):489-500. doi: 10.5664/jcsm.2138. J Clin Sleep Med. 2012. PMID: 23066359 Free PMC article.
-
Sleep apnea is a common and dangerous cardiovascular risk factor.Curr Probl Cardiol. 2025 Jan;50(1):102838. doi: 10.1016/j.cpcardiol.2024.102838. Epub 2024 Sep 4. Curr Probl Cardiol. 2025. PMID: 39242062 Review.
-
Recognition and treatment of sleep-disordered breathing: an important component of chronic disease management.J Transl Med. 2017 May 25;15(1):114. doi: 10.1186/s12967-017-1211-y. J Transl Med. 2017. PMID: 28545542 Free PMC article. Review.
Cited by
-
Inflammatory cytokines tumor necrosis factor-α, interleukin-8 and sleep monitoring in patients with obstructive sleep apnea syndrome.Exp Ther Med. 2019 Mar;17(3):1766-1770. doi: 10.3892/etm.2018.7110. Epub 2018 Dec 18. Exp Ther Med. 2019. PMID: 30783447 Free PMC article.
-
Sleep Apnea Syndrome (SAS) Clinical Practice Guidelines 2020.Sleep Biol Rhythms. 2022 Jan 3;20(1):5-37. doi: 10.1007/s41105-021-00353-6. eCollection 2022 Jan. Sleep Biol Rhythms. 2022. PMID: 38469064 Free PMC article.
-
Treatment of Obstructive Sleep Apnea in Young and Middle-Aged Adults: Effects of Positive Airway Pressure and Compliance on Arterial Stiffness, Endothelial Function, and Cardiac Hemodynamics.J Am Heart Assoc. 2016 Apr 3;5(4):e002930. doi: 10.1161/JAHA.115.002930. J Am Heart Assoc. 2016. PMID: 27039928 Free PMC article.
-
Sleep Disturbances as a Risk Factor for Stroke.J Stroke. 2018 Jan;20(1):12-32. doi: 10.5853/jos.2017.02887. Epub 2018 Jan 31. J Stroke. 2018. PMID: 29402071 Free PMC article. Review.
-
Physiological consequences of CPAP therapy withdrawal in patients with obstructive sleep apnoea-an opportunity for an efficient experimental model.J Thorac Dis. 2018 Jan;10(Suppl 1):S24-S32. doi: 10.21037/jtd.2017.12.142. J Thorac Dis. 2018. PMID: 29445525 Free PMC article. Review.
References
-
- McDaid C, Duree KH, Griffin SC, et al. A systematic review of continuous positive airway pressure for obstructive sleep apnoea-hypopnoea syndrome. Sleep Med Rev. 2009;13:427–36. - PubMed
-
- Marin JM, Carrizo SJ, Vicente E, Agusti AGN. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
