

Pulmonary congestion predicts cardiac events and mortality in ESRD
- PMID: 23449536
- PMCID: PMC3609141
- DOI: 10.1681/ASN.2012100990
Pulmonary congestion predicts cardiac events and mortality in ESRD
Abstract
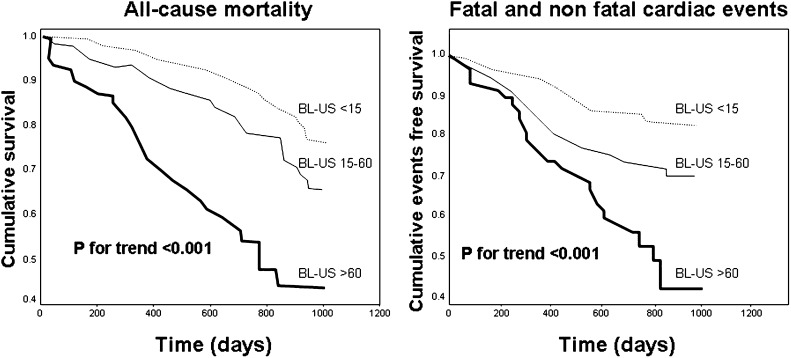
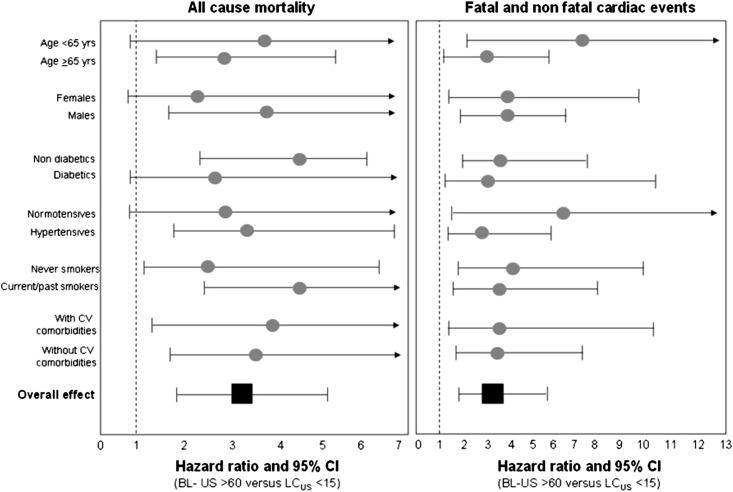
Pulmonary congestion is highly prevalent and often asymptomatic among patients with ESRD treated with hemodialysis, but whether its presence predicts clinical outcomes is unknown. Here, we tested the prognostic value of extravascular lung water measured by a simple, well validated ultrasound B-lines score (BL-US) in a multicenter study that enrolled 392 hemodialysis patients. We detected moderate-to-severe lung congestion in 45% and very severe congestion in 14% of the patients. Among those patients with moderate-to-severe lung congestion, 71% were asymptomatic or presented slight symptoms of heart failure. Compared with those patients having mild or no congestion, patients with very severe congestion had a 4.2-fold risk of death (HR=4.20, 95% CI=2.45-7.23) and a 3.2-fold risk of cardiac events (HR=3.20, 95% CI=1.75-5.88) adjusted for NYHA class and other risk factors. Including the degree of pulmonary congestion in the model significantly improved the risk reclassification for cardiac events by 10% (P<0.015). In summary, lung ultrasound can detect asymptomatic pulmonary congestion in hemodialysis patients, and the resulting BL-US score is a strong, independent predictor of death and cardiac events in this population.
Figures
References
-
- Mees EJ: Volaemia and blood pressure in renal failure: Have old truths been forgotten? Nephrol Dial Transplant 10: 1297–1298, 1995 - PubMed
-
- Moissl UM, Wabel P, Chamney PW, Bosaeus I, Levin NW, Bosy-Westphal A, Korth O, Müller MJ, Ellegård L, Malmros V, Kaitwatcharachai C, Kuhlmann MK, Zhu F, Fuller NJ: Body fluid volume determination via body composition spectroscopy in health and disease. Physiol Meas 27: 921–933, 2006 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
