

The Diagnostic Validity of Clinical Tests in Temporomandibular Internal Derangement: A Systematic Review and Meta-analysis
- PMID: 23449757
- PMCID: PMC3321987
- DOI: 10.3138/ptc.2010-54
The Diagnostic Validity of Clinical Tests in Temporomandibular Internal Derangement: A Systematic Review and Meta-analysis
Abstract
Purpose: To assess the diagnostic validity of clinical tests for temporomandibular internal derangement relative to magnetic resonance imaging (MRI).
Methods: MEDLINE and Embase were searched from 1994 through 2009. Independent reviewers conducted study selection; risk of bias was assessed using Quality Assessment of studies of Diagnostic Accuracy included in Systematic reviews (QUADAS); ≥9/14) and data abstraction. Overall quality of evidence was profiled using Grading of Recommendations Assessment, Development, and Evaluation (GRADE). Agreement was measured using quadratic weighted kappa (κw). Positive (+) or negative (-) likelihood ratios (LR) with 95% CIs were calculated and pooled using the DerSimonian-Laird method and a random-effects model when homogeneous (I(2)≥0.40, Q-test p≤0.10).
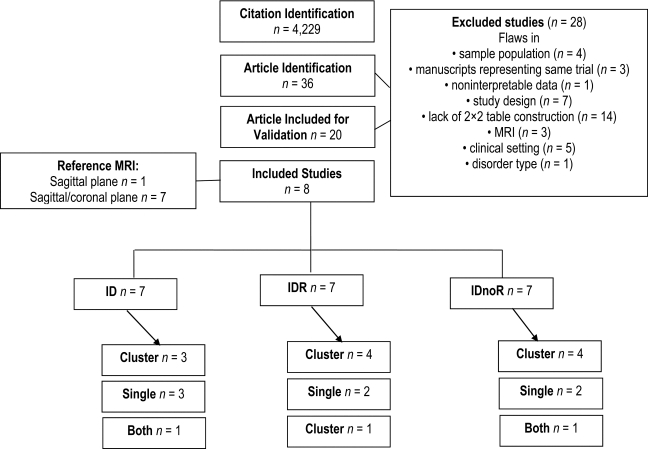
Results: We selected 8 of 36 studies identified. There is very low quality evidence that deflection (+LR: 6.37 [95% CI, 2.13-19.03]) and crepitation (LR:5.88 [95% CI, 1.95-17.76]) as single tests and crepitation, deflection, pain, and limited mouth opening as a cluster of tests are the most valuable for ruling in internal derangement without reduction (+LR:6.37 [95% CI, 2.13-19.03]), (-LR:0.27 [95% CI, 0.11-0.64]) while the test cluster click, deviation, and pain rules out internal derangement with reduction (-LR: 0.09 [95% CI, 0.01-0.72]). No single test or cluster of tests was conclusive and of significant value for ruling in internal derangement with reduction.
Conclusions: Findings of this review will assist clinicians in deciding which diagnostic tests to use when internal derangement is suspected. The literature search revealed a lack of high-quality studies; further research with adequate description of patient populations, blinded assessments, and both sagittal and coronal MRI planes is therefore recommended.
Purpose: To assess the diagnostic validity of clinical tests for temporomandibular internal derangement relative to magnetic resonance imaging (MRI). Methods: MEDLINE and Embase were searched from 1994 through 2009. Independent reviewers conducted study selection; risk of bias was assessed using Quality Assessment of studies of Diagnostic Accuracy included in Systematic reviews (QUADAS); ≥9/14) and data abstraction. Overall quality of evidence was profiled using Grading of Recommendations Assessment, Development, and Evaluation (GRADE). Agreement was measured using quadratic weighted kappa (κw). Positive (+) or negative (−) likelihood ratios (LR) with 95% CIs were calculated and pooled using the DerSimonian–Laird method and a random-effects model when homogeneous (I2≥0.40, Q-test p≤0.10). Results: We selected 8 of 36 studies identified. There is very low quality evidence that deflection (+LR: 6.37 [95% CI, 2.13–19.03]) and crepitation (LR:5.88 [95% CI, 1.95–17.76]) as single tests and crepitation, deflection, pain, and limited mouth opening as a cluster of tests are the most valuable for ruling in internal derangement without reduction (+LR:6.37 [95% CI, 2.13–19.03]), (−LR:0.27 [95% CI, 0.11–0.64]) while the test cluster click, deviation, and pain rules out internal derangement with reduction (−LR: 0.09 [95% CI, 0.01–0.72]). No single test or cluster of tests was conclusive and of significant value for ruling in internal derangement with reduction. Conclusions: Findings of this review will assist clinicians in deciding which diagnostic tests to use when internal derangement is suspected. The literature search revealed a lack of high-quality studies; further research with adequate description of patient populations, blinded assessments, and both sagittal and coronal MRI planes is therefore recommended.
RÉSUMÉ Objectif : Évaluer la validité du diagnostic résultant de tests cliniques en imagerie de résonance magnétique (IRM) pour le dépistage du dérangement interne de l'articulation temporo-mandibulaire (ATM). Méthode : Une recherche a été effectuée dans les bases de données MEDLINE et Embase pour les années 1994 à 2009. Des examinateurs indépendants ont procédé au choix des études répertoriées ; les risques de biais ont été évalués à l'aide de l'échelle QUADAS (Quality Assessment of studies of Diagnostic Accuracy included in Systematic reviews), visant à évaluer la qualité des études sur la fiabilité diagnostique incluses dans les revues systématiques (le pointage obtenu a été ≥9/14) et à l'aide d'abstraction des données. Le profil de la qualité globale des preuves a été établi avec l'échelle GRADE (Grading of Recommendations Assessment, Development, and Evaluation). Le degré d'accord a été mesuré à l'aide du coefficient quadratique kappa pondéré (κw). Les rapports de vraisemblance (RV) positifs (+) ou négatifs (−) avec intervalles de confiance de 95 % ont été calculés et groupés suivant la méthode de DerSimonian–Laird et à l'aide d'un modèle à effets aléatoires lorsque les données étaient homogènes (I2≥0,40, test-Q p≤0,10). Résultats : Nous avons retenu 8 des 36 études identifiées. Les preuves voulant que les tests individuels de déviation (RV+ : 6,37 [95 % IC : 2,13–19,03]) et de crépitation ([RV : 5,88 [95 % IC : 1.95–17.76]) soient fiables étaient de très faible qualité, alors qu'un ensemble de tests regroupant crépitation, déviation, douleur et ouverture limitée de la bouche sont les plus valables au moment de déterminer s'il y a effectivement dérangement interne sans réduction (RV+ : 6,37 [95 % IC : 2,13–19,03]), (RV− : 0,27 (95 % IC : 0,11–0,64]), alors que les tests regroupés – claquement, déviation et douleur – déterminent habituellement s'il y a dérangement interne avec réduction (RV− : 0,09 [95 % IC : 0,01–0,72]). Aucun test unique ni aucun groupe de tests ne semblent avoir de valeur considérable ou significative ni concluante pour déterminer avec précision un dérangement interne avec réduction. Conclusions : Les conclusions de cet examen aideront les cliniciens à décider quels tests diagnostics utiliser lorsqu'ils soupçonnent un dérangement interne. La recherche documentaire a révélé un manque d'études de grande qualité ; des recherches supplémentaires comportant une description adéquate des populations de patients, des évaluations à l'aveugle et des plans sagittaux et coronaires de l'IRM sont donc recommandés.
Keywords: diagnosis; dérangement interne de l'articulation temporo-mandibulaire; imagerie de résonance magnétique; magnetic resonance imaging; predictive value of tests; rapport de vraisemblance positif et négatif; temporomandibular joint disorders; troubles de l'articulation temporo-mandibulaire; valeur prédictive des tests.
Figures
References
-
- Rudisch A, Innerhofer K, Bertram S, et al. Magnetic resonance imaging findings of internal derangement and effusion in patients with unilateral temporomandibular joint pain. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92(5):566–71. doi: . Medline:11709695. - DOI - PubMed
-
- Gross AR. The diagnostic validity of clinical tests in temporomandibular disorders: A systematic overview and meta-analysis. [dissertation] Hamilton (ON): McMaster University; 1994.
-
- Rugh JD, Solberg WK. Oral health status in the United States: temporomandibular disorders. J Dent Educ. 1985;49(6):398–406. Medline:3859518. - PubMed
-
- Greene CS, Marbach JJ. Epidemiologic studies of mandibular dysfunction: a critical review. J Prosthet Dent. 1982;48(2):184–90. doi: . Medline:7050363. - DOI - PubMed
-
- Rasmussen OC. Description of population and progress of symptoms in a longitudinal study of temporomandibular arthropathy. Scand J Dent Res. 1981;89(2):196–203. Medline:6943666. - PubMed
LinkOut - more resources
Full Text Sources