

Evaluation of a noninvasive algorithm for differentiation of obstructive and central hypopneas
- PMID: 23450252
- PMCID: PMC3571737
- DOI: 10.5665/sleep.2450
Evaluation of a noninvasive algorithm for differentiation of obstructive and central hypopneas
Abstract
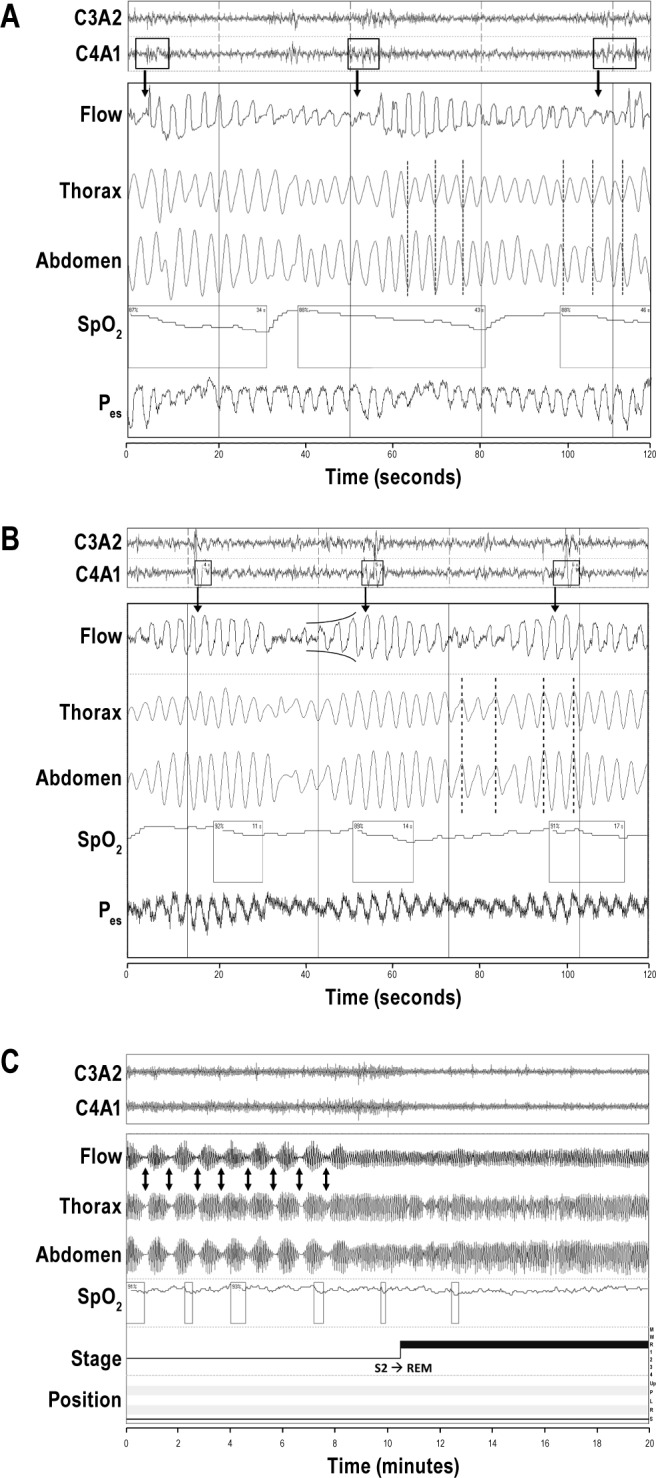
Study objectives: The clear discrimination of central and obstructive hypopneas is highly relevant to avoid misinterpretation and inappropriate treatment of complicated breathing patterns. Esophageal manometry is the accepted standard for the differentiation of the phenotypes of sleep apnea. However, it is limited in its use due to poor acceptance by patients and therefore rarely performed in routine clinical practice. Flattening of the inspiratory airflow curve, paradoxical breathing, arousal position, sleep stages, and breathing pattern at the end of the hypopnea can each give hints for the classification of hypopnea. The aim of this study was to evaluate a standardized algorithm combining these polysomnographic parameters for the discrimination of hypopneas in everyday practice.
Methods: Polysomnography (PSG) and esophageal manometry were performed in 41 patients suspected of having sleep apnea (33 male, 52.3 ± 15.9 yr, body mass index 28.6 ± 4.5 kg/m(2)). Hypopneas were independently discriminated by blinded investigators based on esophageal pressure and the PSG-based algorithm. Only those hypopneas that could be differentiated with both methods were evaluated.
Results: There were 1,175 of 1,837 hypopneas (64%) that could be defined by esophageal pressure, 1,812 (98.6%) by the PSG-based algorithm. Using esophageal pressure as a reference, the new algorithm correctly defined 76.9% of central and 60.5% of obstructive hypopneas. The overall accuracy was 68%. The isolated analysis of single PSG parameters revealed a lower accuracy compared with the combined algorithm.
Conclusions: The PSG-based algorithm allows for discrimination of most hypopneas. It is advantageous in comparison with esophageal pressure because it is noninvasive and less impaired by artefacts. Therefore, it is a potentially helpful tool for sleep specialists.
Citation: Randerath WJ; Treml M; Priegnitz C; Stieglitz S; Hagmeyer L; Morgenstern C. Evaluation of a noninvasive algorithm for differentiation of obstructive and central hypopneas. SLEEP 2013;36(3):363-368.
Keywords: Arousal; NREM sleep; REM sleep; crescendo pattern; esophageal pressure; flattening; paradoxical breathing; plethysmography.
Figures

Comment in
-
Are we ready to define central hypopneas?Sleep. 2013 Mar 1;36(3):305-6. doi: 10.5665/sleep.2434. Sleep. 2013. PMID: 23450900 Free PMC article. No abstract available.
References
-
- Iber C, Ancoli-Israel S, Chesson AL, Quan SF. 1st ed. Westchester, Illinois: American academy of Sleep Medicine; 2007. The AASM manual for the scoring of sleep and associated events: Rules, Technology and Technical Specifications.
-
- Morgenthaler TI, Kagramanov V, Hanak V, Decker PA. Complex sleep apnea syndrome: is it a unique clinical syndrome? Sleep. 2006;29:1203–9. - PubMed
-
- Javaheri S. CPAP should not be used for central sleep apnea in congestive heart failure patients. J Clin Sleep Med. 2006;2:399–402. - PubMed
-
- Javaheri S, Caref EB, Chen E, Tong KB, Abraham WT. Sleep apnea testing and outcomes in a large cohort of Medicare beneficiaries with newly diagnosed heart failure. Am J Respir Crit Care Med. 2011;183:539–46. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
