

Serologic vaccination response after solid organ transplantation: a systematic review
- PMID: 23451126
- PMCID: PMC3579937
- DOI: 10.1371/journal.pone.0056974
Serologic vaccination response after solid organ transplantation: a systematic review
Abstract
Background: Infectious diseases after solid organ transplantation (SOT) are one of the major complications in transplantation medicine. Vaccination-based prevention is desirable, but data on the response to active vaccination after SOT are conflicting.
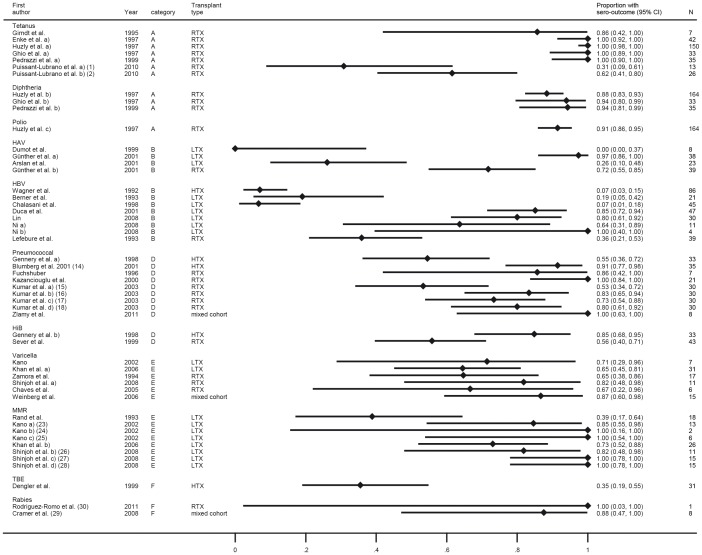
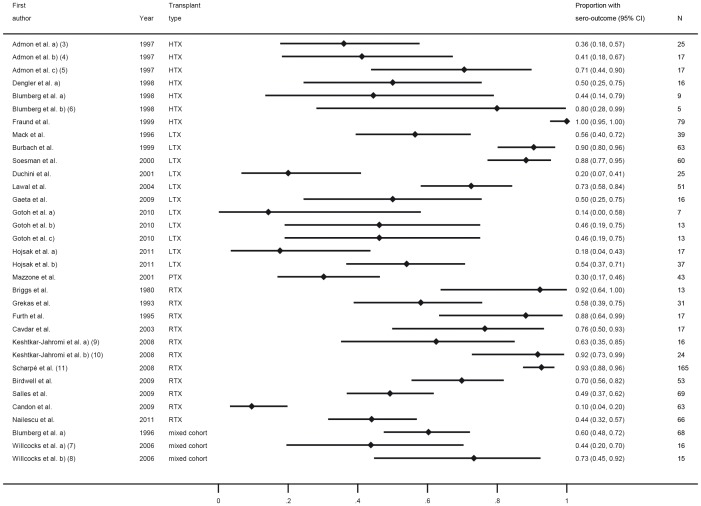
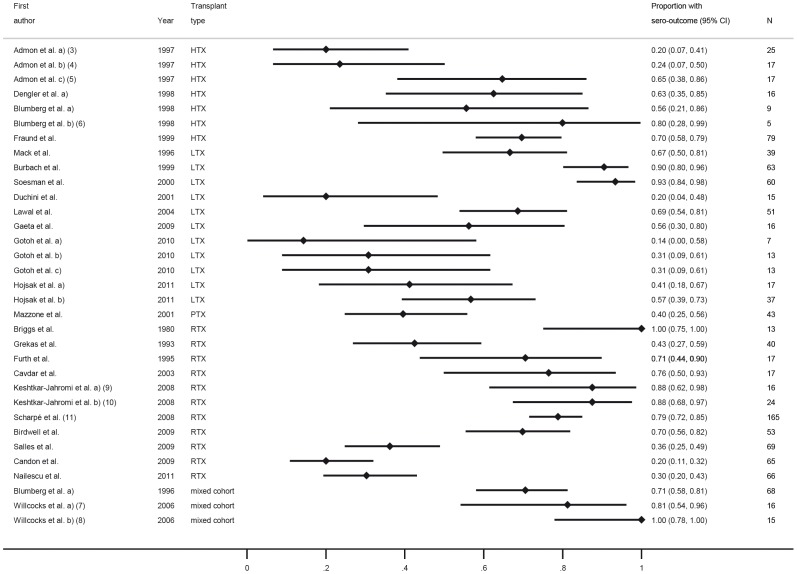
Methods: In this systematic review, we identify the serologic response rate of SOT recipients to post-transplantation vaccination against tetanus, diphtheria, polio, hepatitis A and B, influenza, Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitides, tick-borne encephalitis, rabies, varicella, mumps, measles, and rubella.
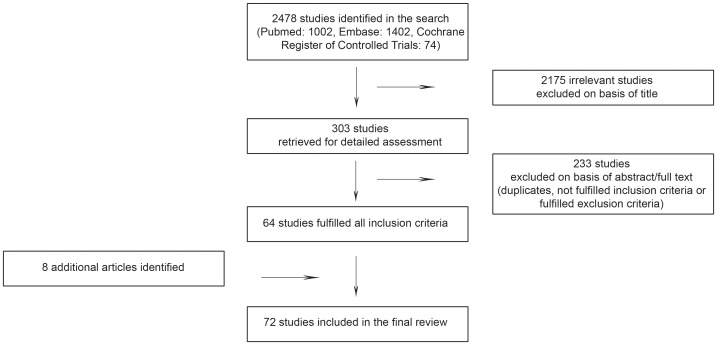
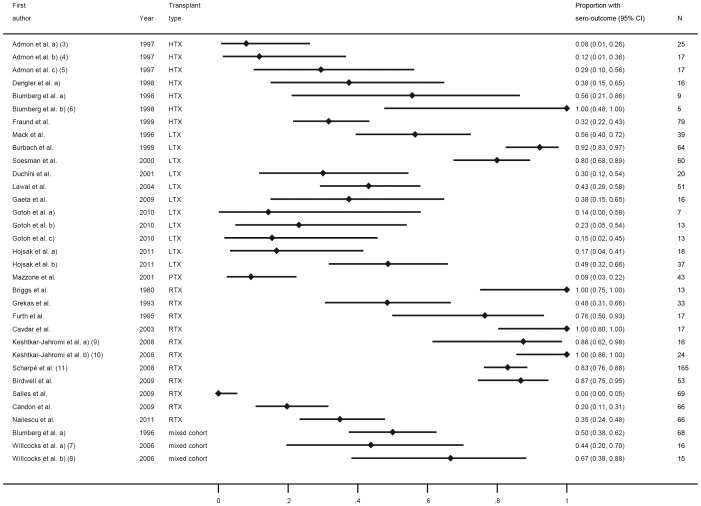
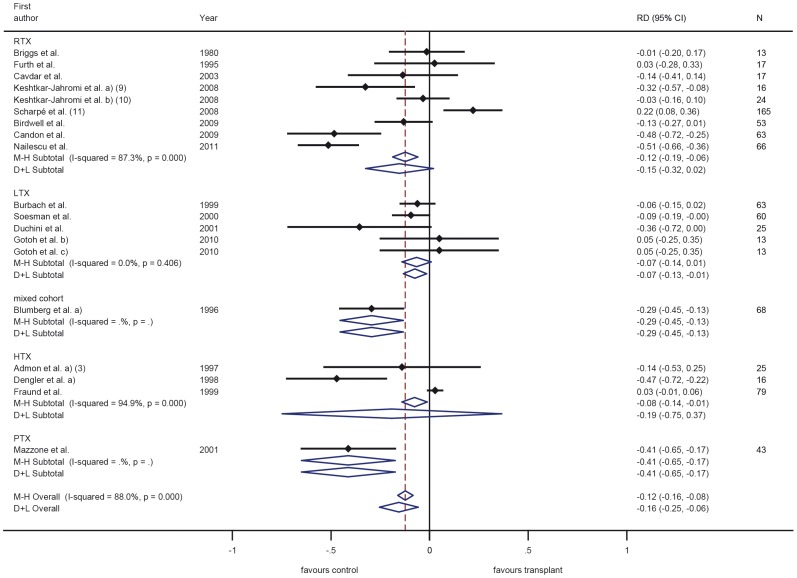
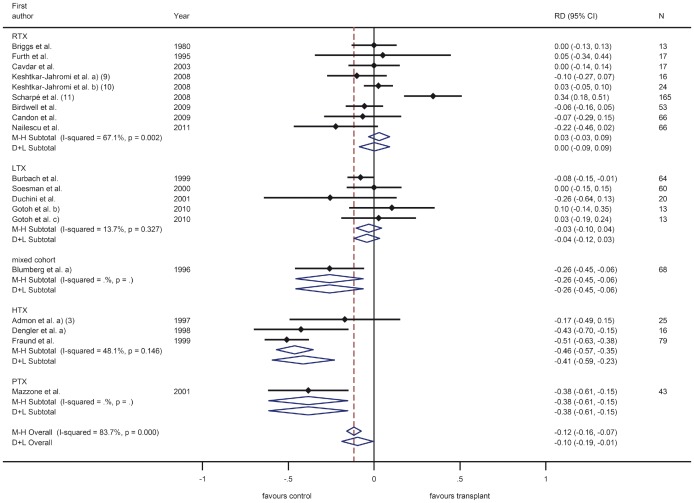
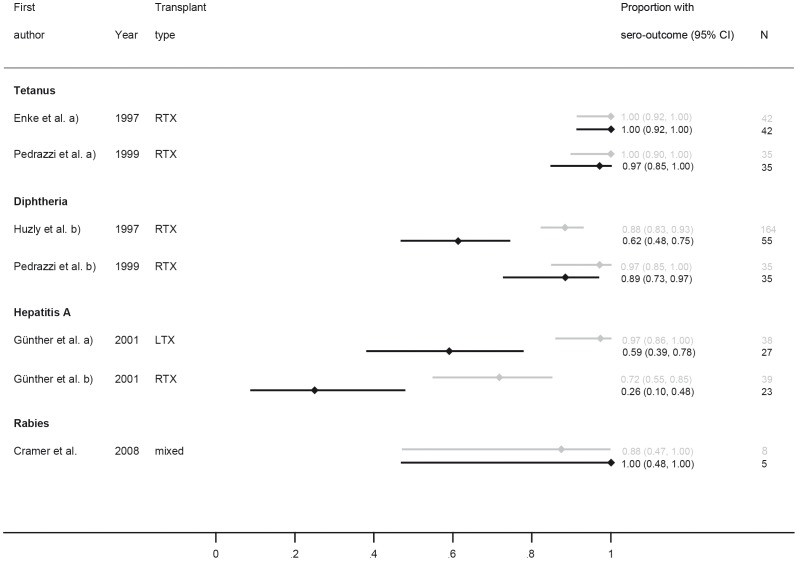
Results: Of the 2478 papers initially identified, 72 were included in the final review. The most important findings are that (1) most clinical trials conducted and published over more than 30 years have all been small and highly heterogeneous regarding trial design, patient cohorts selected, patient inclusion criteria, dosing and vaccination schemes, follow up periods and outcomes assessed, (2) the individual vaccines investigated have been studied predominately only in one group of SOT recipients, i.e. tetanus, diphtheria and polio in RTX recipients, hepatitis A exclusively in adult LTX recipients and mumps, measles and rubella in paediatric LTX recipients, (3) SOT recipients mount an immune response which is for most vaccines lower than in healthy controls. The degree to which this response is impaired varies with the type of vaccine, age and organ transplanted and (4) for some vaccines antibodies decline rapidly.
Conclusion: Vaccine-based prevention of infectious diseases is far from satisfactory in SOT recipients. Despite the large number of vaccination studies preformed over the past decades, knowledge on vaccination response is still limited. Even though the protection, which can be achieved in SOT recipients through vaccination, appears encouraging on the basis of available data, current vaccination guidelines and recommendations for post-SOT recipients remain poorly supported by evidence. There is an urgent need to conduct appropriately powered vaccination trials in well-defined SOT recipient cohorts.
Conflict of interest statement
Figures

References
-
- Grossi PA, Costa AN, Fehily D, Blumberg EA, Kuehnert MJ, et al. (2012) Infections and organ transplantation: new challenges for prevention and treatment–a colloquium. Transplantation 93: S4–S39. - PubMed
-
- Fishman JA (2011) Infections in immunocompromised hosts and organ transplant recipients: essentials. Liver Transpl 17 Suppl 3S34–37. - PubMed
-
- Gentile G, Foa R (2011) Viral infections associated with the clinical use of monoclonal antibodies. Clin Microbiol Infect 17: 1769–1775. - PubMed
-
- Plotkin SL, Plotkin SA (2008) A short history of vaccination. In: Plotkin SA, Orenstein WA, Offit PA, editors. Vaccines. Saunders Elsevier. 1–16.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
