

Cost-effectiveness of additional catheter-directed thrombolysis for deep vein thrombosis
- PMID: 23452204
- PMCID: PMC4027959
- DOI: 10.1111/jth.12184
Cost-effectiveness of additional catheter-directed thrombolysis for deep vein thrombosis
Abstract
Background: Additional treatment with catheter-directed thrombolysis (CDT) has recently been shown to reduce post-thrombotic syndrome (PTS).
Objectives: To estimate the cost effectiveness of additional CDT compared with standard treatment alone.
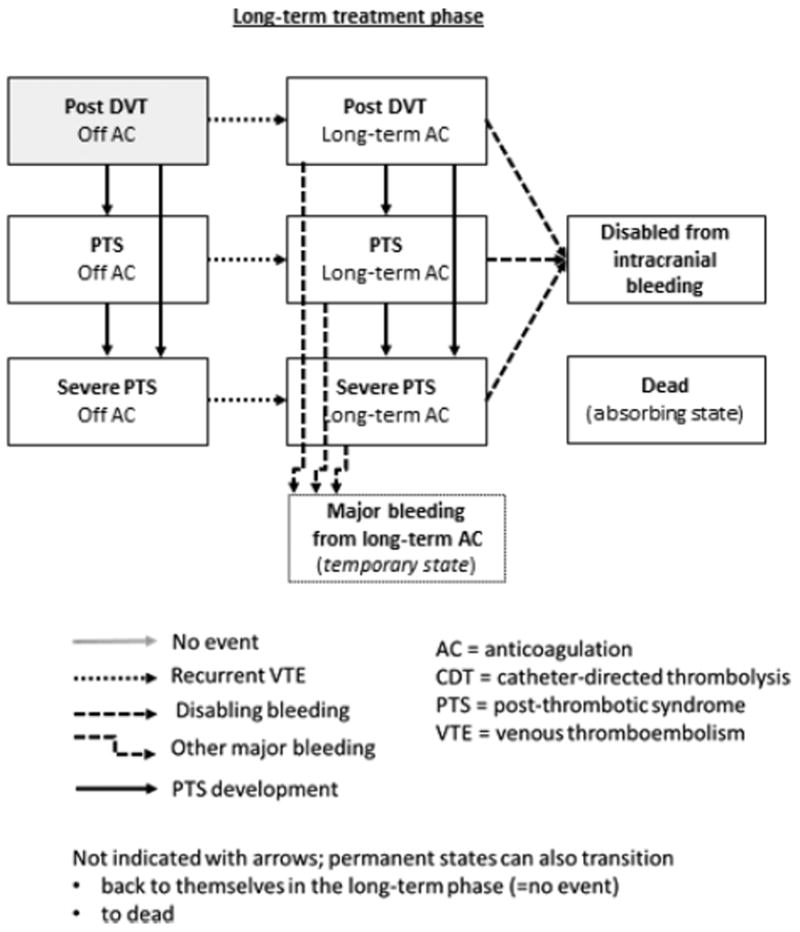
Methods: Using a Markov decision model, we compared the two treatment strategies in patients with a high proximal deep vein thrombosis (DVT) and a low risk of bleeding. The model captured the development of PTS, recurrent venous thromboembolism and treatment-related adverse events within a lifetime horizon and the perspective of a third-party payer. Uncertainty was assessed with one-way and probabilistic sensitivity analyzes. Model inputs from the CaVenT study included PTS development, major bleeding from CDT and utilities for post DVT states including PTS. The remaining clinical inputs were obtained from the literature. Costs obtained from the CaVenT study, hospital accounts and the literature are expressed in US dollars ($); effects in quality adjusted life years (QALY).
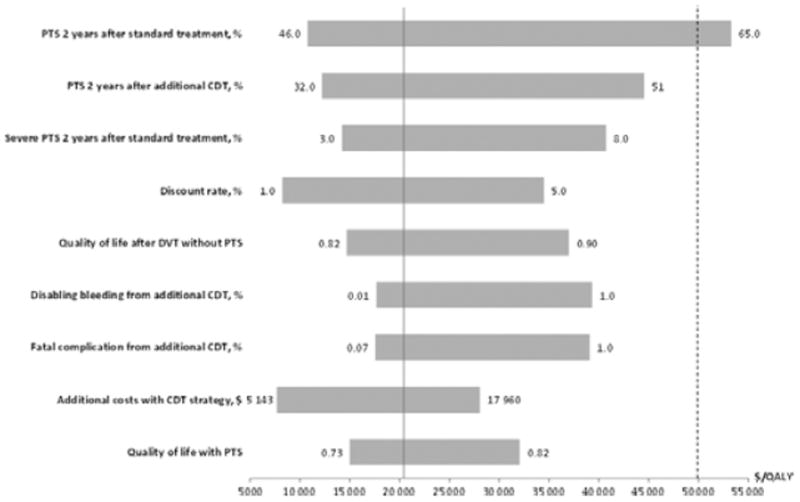
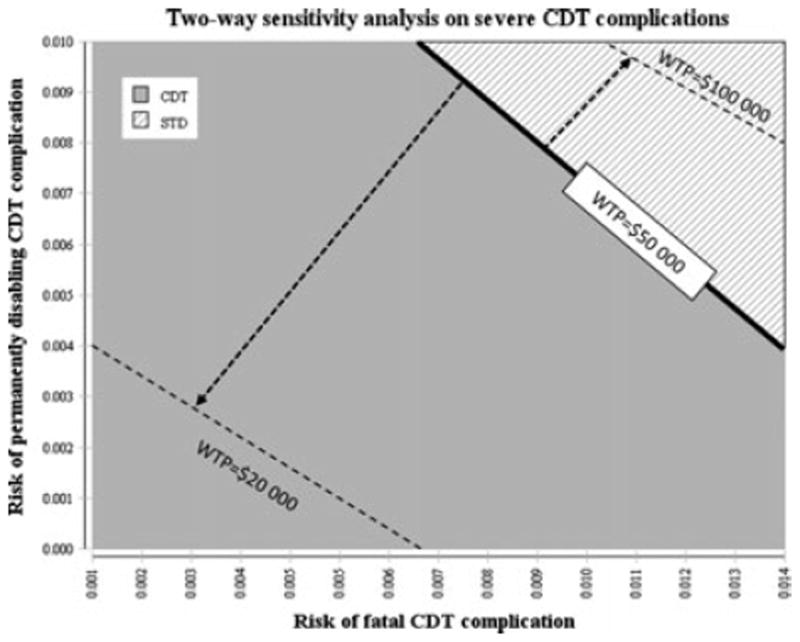
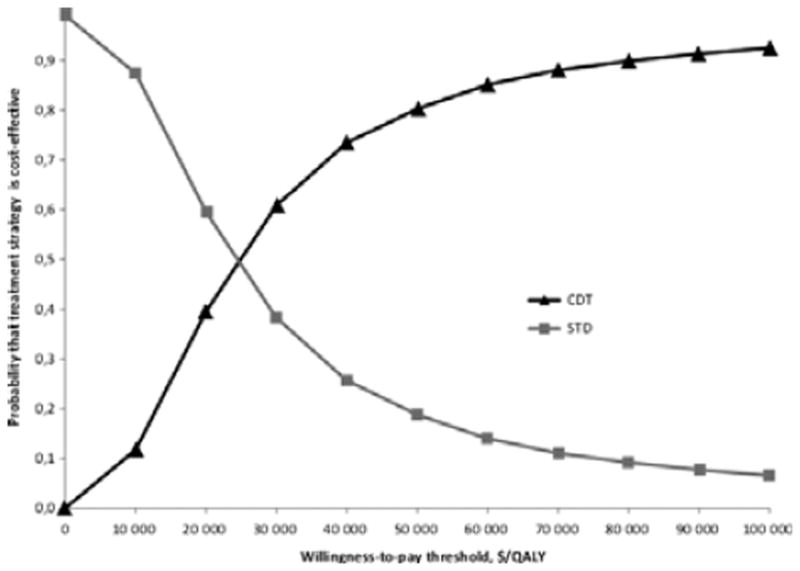
Results: In base case analyzes, additional CDT accumulated 32.31 QALYs compared with 31.68 QALYs after standard treatment alone. Direct medical costs were $64,709 for additional CDT and $51,866 for standard treatment. The incremental cost-effectiveness ratio (ICER) was $20,429/QALY gained. One-way sensitivity analysis showed model sensitivity to the clinical efficacy of both strategies, but the ICER remained < $55,000/QALY over the full range of all parameters. The probability that CDT is cost effective was 82% at a willingness to pay threshold of $50,000/QALY gained.
Conclusions: Additional CDT is likely to be a cost-effective alternative to the standard treatment for patients with a high proximal DVT and a low risk of bleeding.
Keywords: anticoagulation; cost-effectiveness analysis; decision model; post-thrombotic syndrome; thrombolytic therapy; venous thrombosis.
© 2013 International Society on Thrombosis and Haemostasis.
Conflict of interest statement
The authors state that they have no conflict of interests.
Figures
Comment in
-
Catheter-directed thrombolysis for deep venous thrombosis might be cost-effective, but for whom?J Thromb Haemost. 2013 Jun;11(6):1029-31. doi: 10.1111/jth.12246. J Thromb Haemost. 2013. PMID: 23581286 No abstract available.
References
-
- Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, Nelson ME, Wells PS, Gould MK, Dentali F, Crowther M, Kahn SR American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:e419S–94S. - PMC - PubMed
-
- Prandoni P, Lensing AW, Prins MH, Frulla M, Marchiori A, Bernardi E, Tormene D, Mosena L, Pagnan A, Girolami A. Below-knee elastic compression stockings to prevent the post-thrombotic syndrome: a randomized, controlled trial. Ann Intern Med. 2004;141:249–56. - PubMed
-
- Brandjes DP, Büller HR, Heijboer H, Huisman MV, de Rijk M, Jagt H, ten Cate JW. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet. 1997;349:759–62. - PubMed
-
- Kahn SR, Shrier I, Julian JA, Ducruet T, Arsenault L, Miron MJ, Roussin A, Desmarais S, Joyal F, Kassis J, Solymoss S, Desjardins L, Lamping DL, Johri M, Ginsberg JS. Determinants and time course of the postthrombotic syndrome after acute deep venous thrombosis. Ann Intern Med. 2008;149:698–707. - PubMed
-
- Guanella R, Ducruet T, Johri M, Miron MJ, Roussin A, Desmarais S, Joyal F, Kassis J, Solymoss S, Ginsberg JS, Lamping DL, Shrier I, Kahn SR. Economic burden and cost determinants of deep vein thrombosis during two years following diagnosis: a prospective evaluation. J Thromb Haemost. 2011;9:2397–405. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
