

Diabetes, perioperative ischaemia and volatile anaesthetics: consequences of derangements in myocardial substrate metabolism
- PMID: 23452502
- PMCID: PMC3599199
- DOI: 10.1186/1475-2840-12-42
Diabetes, perioperative ischaemia and volatile anaesthetics: consequences of derangements in myocardial substrate metabolism
Abstract
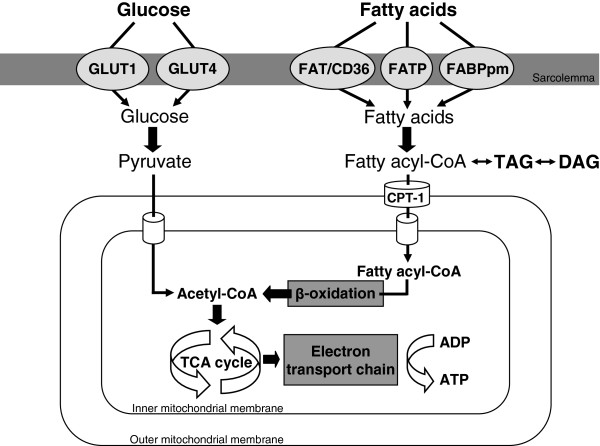
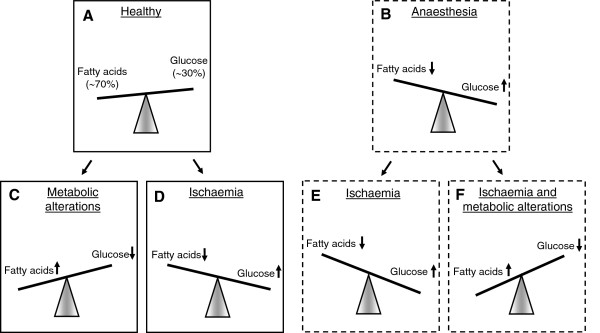
Volatile anaesthetics exert protective effects on the heart against perioperative ischaemic injury. However, there is growing evidence that these cardioprotective properties are reduced in case of type 2 diabetes mellitus. A strong predictor of postoperative cardiac function is myocardial substrate metabolism. In the type 2 diabetic heart, substrate metabolism is shifted from glucose utilisation to fatty acid oxidation, resulting in metabolic inflexibility and cardiac dysfunction. The ischaemic heart also loses its metabolic flexibility and can switch to glucose or fatty acid oxidation as its preferential state, which may deteriorate cardiac function even further in case of type 2 diabetes mellitus.Recent experimental studies suggest that the cardioprotective properties of volatile anaesthetics partly rely on changing myocardial substrate metabolism. Interventions that target at restoration of metabolic derangements, like lifestyle and pharmacological interventions, may therefore be an interesting candidate to reduce perioperative complications. This review will focus on the current knowledge regarding myocardial substrate metabolism during volatile anaesthesia in the obese and type 2 diabetic heart during perioperative ischaemia.
Figures
References
-
- Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleischmann KE, Freeman WK, Froehlich JB, Kasper EK, Kersten JR, Riegel B, Robb JF, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Buller CE, Creager MA, Ettinger SM, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Hunt SA. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the american college of cardiology/american heart association task force on practice guidelines (writing committee to revise the,guidelines on perioperative cardiovascular evaluation for noncardiac surgery): developed in collaboration with the american society of echocardiography, american society of nuclear cardiology, heart rhythm society, society of cardiovascular anesthesiologists, society for cardiovascular angiography and interventions, society for vascular medicine and biology, and society for vascular surgery. Circulation. 2002;2007(116):e418–e499. - PubMed
-
- Gupta PK, Gupta H, Sundaram A, Kaushik M, Fang X, Miller WJ, Esterbrooks DJ, Hunter CB, Pipinos II, Johanning JM, Lynch TG, Forse RA, Mohiuddin SM, Mooss AN. Development and validation of a risk calculator for prediction of cardiac risk after surgery. Circulation. 2011;124:381–387. doi: 10.1161/CIRCULATIONAHA.110.015701. - DOI - PubMed
-
- Unwin N, Whiting D, Guariguata L, Hennis A, Husseini A, Ji L, Kissimova-Skarbek K, Libman I, Mayer-Davis E, Motala A, Narayan V, Ramachandran A, Roglic G, Sham J, Wareham N, Zhang P. IDF diabetes atlas 2011. 5. Brussels: International Diabetes Federation; 2011.
-
- Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, Sugarbaker DJ, Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100:1043–1049. doi: 10.1161/01.CIR.100.10.1043. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
