

Eosinophilic esophagitis
- PMID: 23452635
- PMCID: PMC3589114
- DOI: 10.1016/j.gtc.2012.11.008
Eosinophilic esophagitis
Abstract
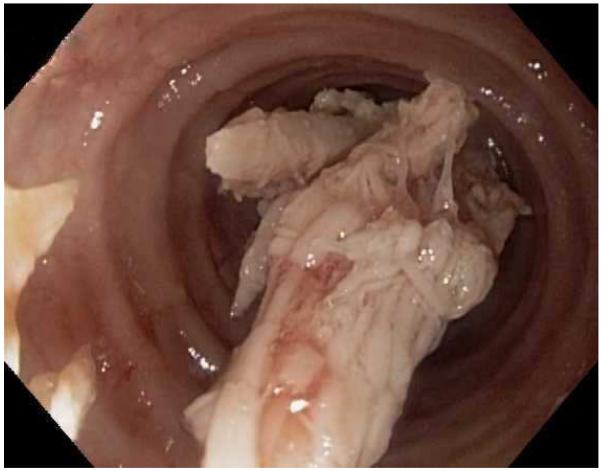
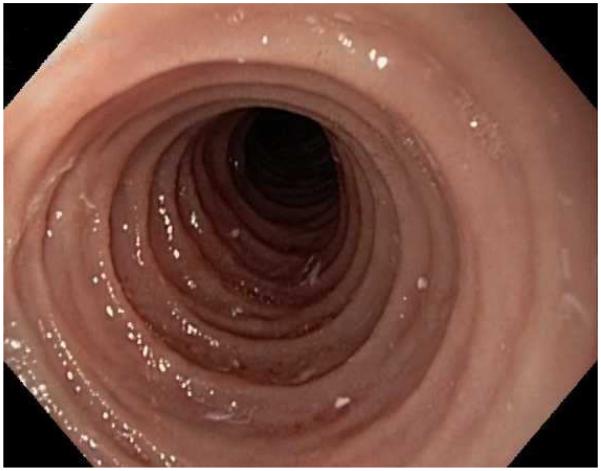
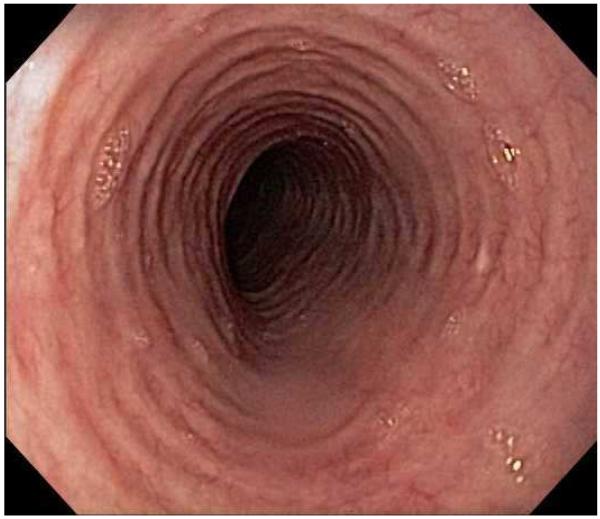
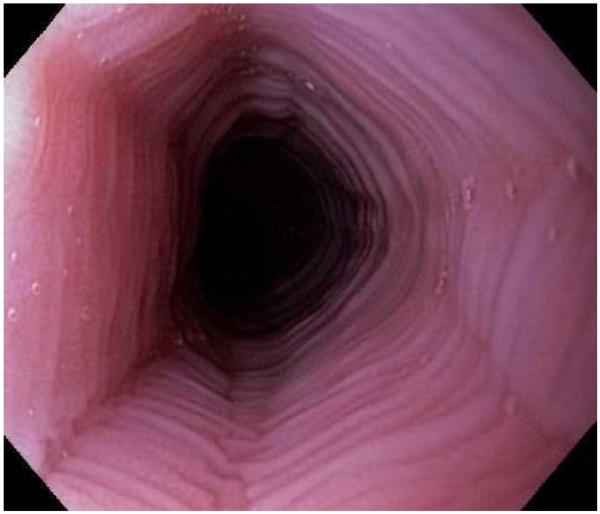
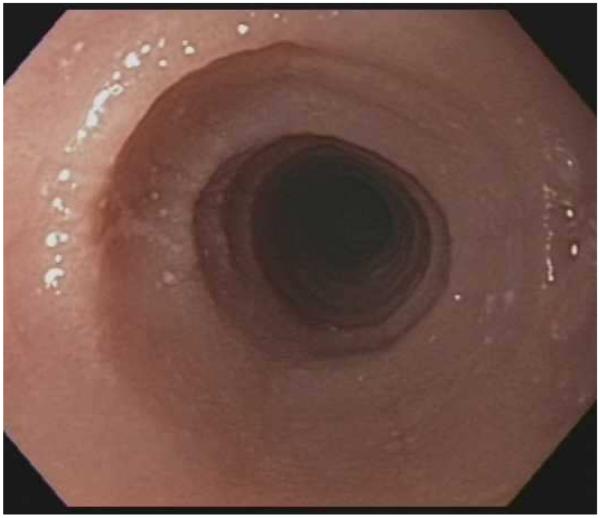
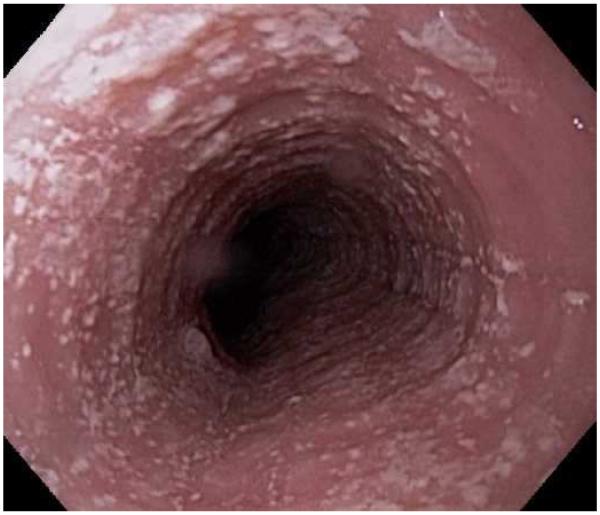
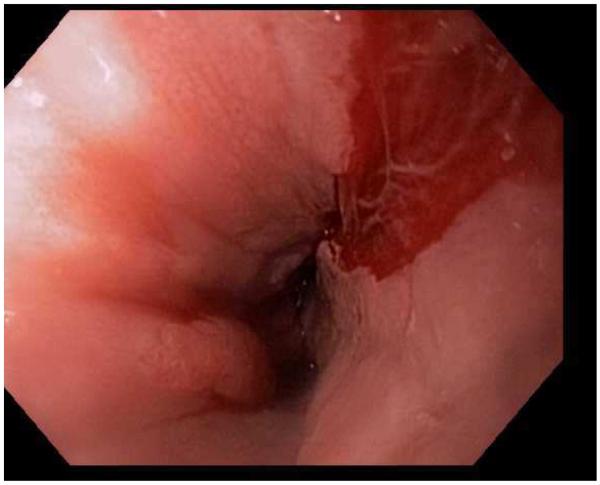
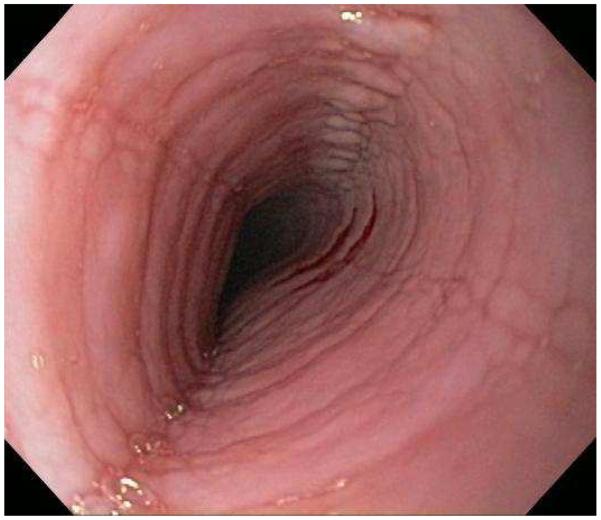
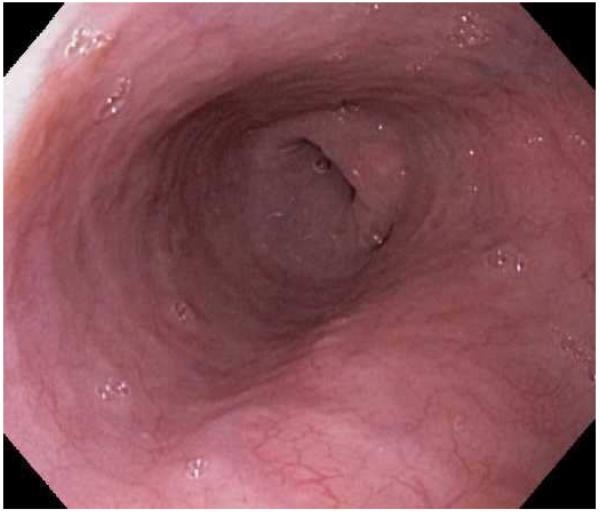
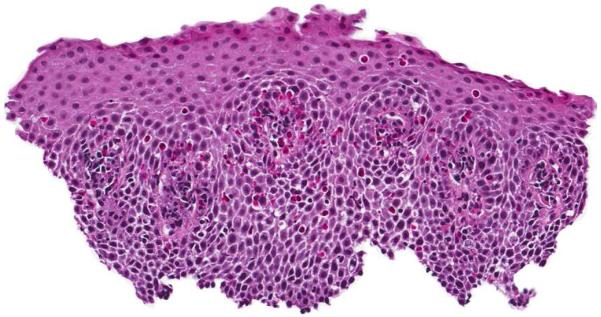
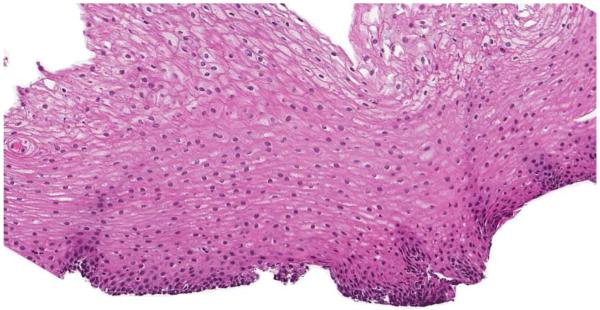
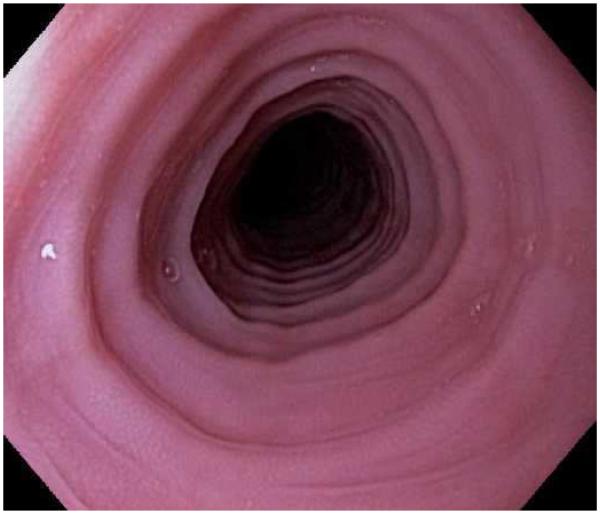
Eosinophilic esophagitis (EoE) is a chronic immune-mediated condition whereby infiltration of eosinophils into the esophageal mucosa leads to symptoms of esophageal dysfunction. EoE is encountered in a substantial proportion of patients undergoing diagnostic upper endoscopy. This review discusses the clinical, endoscopic, and histologic features of EoE and presents the most recent guidelines for its diagnosis. Selected diagnostic dilemmas are described, including distinguishing EoE from gastroesophageal reflux disease and addressing the newly recognized clinical entity of proton-pump inhibitor-responsive esophageal eosinophilia. Also highlighted is evidence to support both pharmacologic and nonpharmacologic treatments, including topical corticosteroids, dietary elimination therapy, and endoscopic dilation.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures





References
-
- Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128:3–20.e6. - PubMed
-
- Landres RT, Kuster GG, Strum WB. Eosinophilic esophagitis in a patient with vigorous achalasia. Gastroenterology. 1978;74:1298–301. - PubMed
-
- Attwood SE, Smyrk TC, Demeester TR, Jones JB. Esophageal eosinophilia with dysphagia. A distinct clinicopathologic syndrome. Dig Dis Sci. 1993;38:109–16. - PubMed
-
- Straumann A, Spichtin HP, Bernoulli R, Loosli J, Vogtlin J. Idiopathic eosinophilic esophagitis: a frequently overlooked disease with typical clinical aspects and discrete endoscopic findings. Schweiz Med Wochenschr. 1994;124:1419–29. - PubMed
-
- Kelly KJ, Lazenby AJ, Rowe PC, Yardley JH, Perman JA, Sampson HA. Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula. Gastroenterology. 1995;109:1503–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
