

Effects of unconditional and conditional cash transfers on child health and development in Zimbabwe: a cluster-randomised trial
- PMID: 23453283
- PMCID: PMC3627205
- DOI: 10.1016/S0140-6736(12)62168-0
Effects of unconditional and conditional cash transfers on child health and development in Zimbabwe: a cluster-randomised trial
Abstract
Background: Cash-transfer programmes can improve the wellbeing of vulnerable children, but few studies have rigorously assessed their effectiveness in sub-Saharan Africa. We investigated the effects of unconditional cash transfers (UCTs) and conditional cash transfers (CCTs) on birth registration, vaccination uptake, and school attendance in children in Zimbabwe.
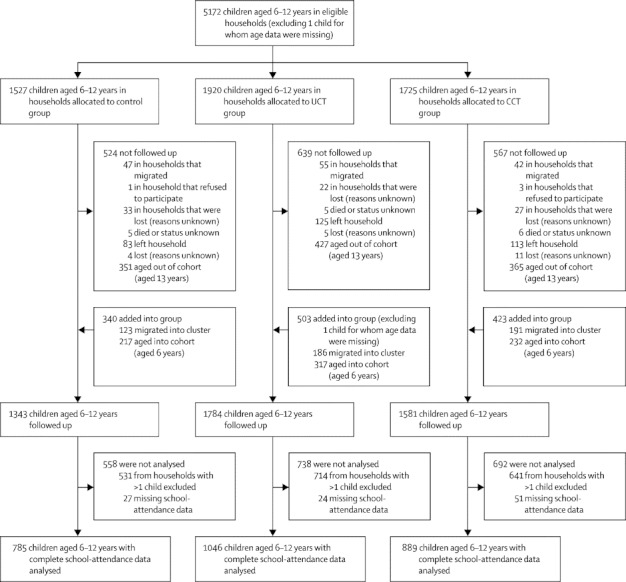
Methods: We did a matched, cluster-randomised controlled trial in ten sites in Manicaland, Zimbabwe. We divided each study site into three clusters. After a baseline survey between July, and September, 2009, clusters in each site were randomly assigned to UCT, CCT, or control, by drawing of lots from a hat. Eligible households contained children younger than 18 years and satisfied at least one other criteria: head of household was younger than 18 years; household cared for at least one orphan younger than 18 years, a disabled person, or an individual who was chronically ill; or household was in poorest wealth quintile. Between January, 2010, and January, 2011, households in UCT clusters collected payments every 2 months. Households in CCT clusters could receive the same amount but were monitored for compliance with several conditions related to child wellbeing. Eligible households in all clusters, including control clusters, had access to parenting skills classes and received maize seed and fertiliser in December, 2009, and August, 2010. Households and individuals delivering the intervention were not masked, but data analysts were. The primary endpoints were proportion of children younger than 5 years with a birth certificate, proportion younger than 5 years with up-to-date vaccinations, and proportion aged 6-12 years attending school at least 80% of the time. This trial is registered with ClinicalTrials.gov, number NCT00966849.
Findings: 1199 eligible households were allocated to the control group, 1525 to the UCT group, and 1319 to the CCT group. Compared with control clusters, the proportion of children aged 0-4 years with birth certificates had increased by 1·5% (95% CI -7·1 to 10·1) in the UCT group and by 16·4% (7·8-25·0) in the CCT group by the end of the intervention period. The proportions of children aged 0-4 years with complete vaccination records was 3·1% (-3·8 to 9·9) greater in the UCT group and 1·8% (-5·0 to 8·7) greater in the CCT group than in the control group. The proportions of children aged 6-12 years who attended school at least 80% of the time was 7·2% (0·8-13·7) higher in the UCT group and 7·6% (1·2-14·1) in the CCT group than in the control group.
Interpretation: Our results support strategies to integrate cash transfers into social welfare programming in sub-Saharan Africa, but further evidence is needed for the comparative effectiveness of UCT and CCT programmes in this region.
Funding: Wellcome Trust, the World Bank through the Partnership for Child Development, and the Programme of Support for the Zimbabwe National Action Plan for Orphans and Vulnerable Children.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures




Comment in
-
Cash-transfer programmes in developing countries.Lancet. 2013 Apr 13;381(9874):1254-5. doi: 10.1016/S0140-6736(13)60358-X. Lancet. 2013. PMID: 23582384 No abstract available.
References
-
- Shibuya K. Conditional cash transfer: a magic bullet for health? Lancet. 2008;371:789–791. - PubMed
-
- Fiszbein A, Schady N. Conditional cash transfers: reducing present and future poverty. World Bank; Washington, DC: 2009.
-
- Nyamukapa C, Gregson S. Extended family's and women's roles in safeguarding orphans' education in AIDS-afflicted rural Zimbabwe. Social Sci Med. 2005;60:2155–2167. - PubMed
-
- de Brauw A, Hoddinott J. Must conditional cash transfer programs be conditioned to be effective? The impact of conditioning transfers on school enrollment in Mexico. International Food Policy Research Institute; Washington, DC: 2007.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
