

Efficacy of RTS,S malaria vaccines: individual-participant pooled analysis of phase 2 data
- PMID: 23454164
- PMCID: PMC3771416
- DOI: 10.1016/S1473-3099(13)70005-7
Efficacy of RTS,S malaria vaccines: individual-participant pooled analysis of phase 2 data
Erratum in
- Lancet Infect Dis. 2013 Sep;13(9):735
Abstract
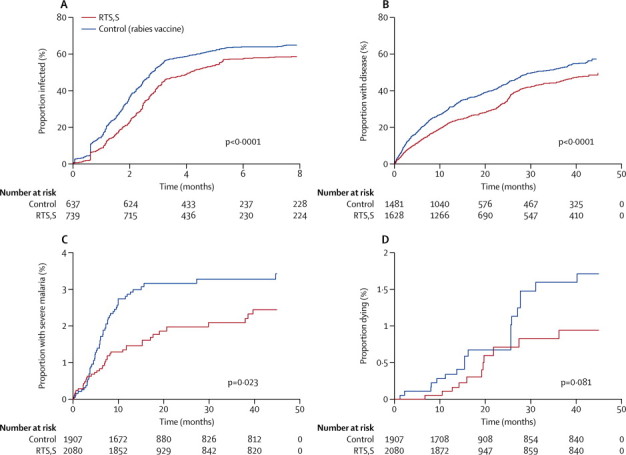
Background: The efficacy of RTS,S/AS01 as a vaccine for malaria is being tested in a phase 3 clinical trial. Early results show significant, albeit partial, protection against clinical malaria and severe malaria. To ascertain variations in vaccine efficacy according to covariates such as transmission intensity, choice of adjuvant, age at vaccination, and bednet use, we did an individual-participant pooled analysis of phase 2 clinical data.
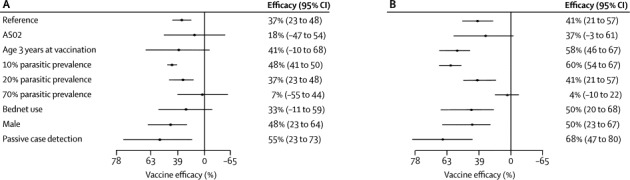
Methods: We analysed data from 11 different sites in Africa, including 4453 participants. We measured heterogeneity in vaccine efficacy by estimating the interactions between covariates and vaccination in pooled multivariable Cox regression and Poisson regression analyses. Endpoints for measurement of vaccine efficacy were infection, clinical malaria, severe malaria, and death. We defined transmission intensity levels according to the estimated local parasite prevalence in children aged 2-10 years (PrP₂₋₁₀), ranging from 5% to 80%. Choice of adjuvant was either AS01 or AS02.
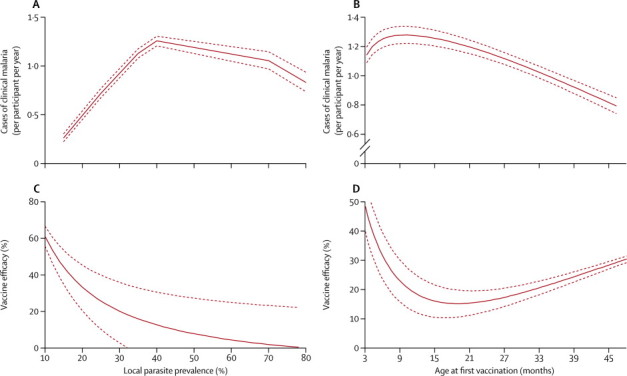
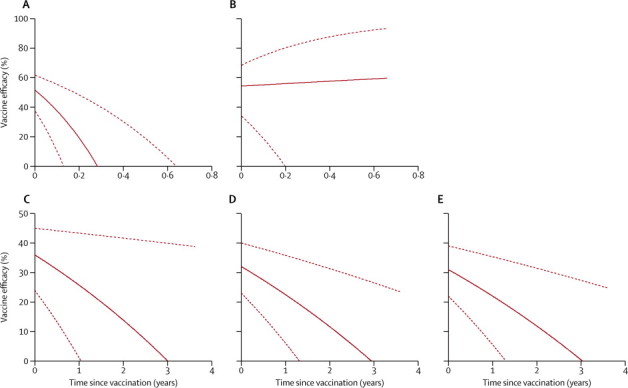
Findings: Vaccine efficacy against all episodes of clinical malaria varied by transmission intensity (p=0·001). At low transmission (PrP₂₋₁₀ 10%) vaccine efficacy was 60% (95% CI 54 to 67), at moderate transmission (PrP₂₋₁₀ 20%) it was 41% (21 to 57), and at high transmission (PrP₂₋₁₀ 70%) the efficacy was 4% (-10 to 22). Vaccine efficacy also varied by adjuvant choice (p<0·0001)--eg, at low transmission (PrP₂₋₁₀ 10%), efficacy varied from 60% (95% CI 54 to 67) for AS01 to 47% (14 to 75) for AS02. Variations in efficacy by age at vaccination were of borderline significance (p=0·038), and bednet use and sex were not significant covariates. Vaccine efficacy (pooled across adjuvant choice and transmission intensity) varied significantly (p<0·0001) according to time since vaccination, from 36% efficacy (95% CI 24 to 45) at time of vaccination to 0% (-38 to 38) after 3 years.
Interpretation: Vaccine efficacy against clinical disease was of limited duration and was not detectable 3 years after vaccination. Furthermore, efficacy fell with increasing transmission intensity. Outcomes after vaccination cannot be gauged accurately on the basis of one pooled efficacy figure. However, predictions of public-health outcomes of vaccination will need to take account of variations in efficacy by transmission intensity and by time since vaccination.
Funding: Medical Research Council (UK); Bill & Melinda Gates Foundation Vaccine Modelling Initiative; Wellcome Trust.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Assessment of the RTS,S/AS01 malaria vaccine.Lancet Infect Dis. 2013 Apr;13(4):280-2. doi: 10.1016/S1473-3099(13)70047-1. Epub 2013 Mar 1. Lancet Infect Dis. 2013. PMID: 23454165 No abstract available.
References
-
- The RTS,S Clinical Trials Partnership First results of phase 3 trial of RTS,S/AS01 malaria vaccine in African children. N Engl J Med. 2011;365:1863–1875. - PubMed
-
- Kester KE, Cummings JF, Ofori-Anyinam O. Randomized, double-blind, phase 2a trial of falciparum malaria vaccines RTS,S/AS01B and RTS,S/AS02A in malaria-naive adults: safety, efficacy, and immunologic associates of protection. J Infect Dis. 2009;200:337–346. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
