

Bioavailability of IgG administered by the subcutaneous route
- PMID: 23456255
- PMCID: PMC3682093
- DOI: 10.1007/s10875-013-9876-3
Bioavailability of IgG administered by the subcutaneous route
Abstract
Purpose: US licensing studies of subcutaneous IgG (SCIG) calculate dose adjustments necessary to achieve area under the curve (AUC) of serum IgG vs. time on SCIG that is non-inferior to that on intravenous IgG (IVIG), within the FDA-set limit of ±20%. The results are interpreted as showing that different SCIGs differ in bioavailability. We used three approaches to determine if the bioavailabilities were actually different.
Methods: Dose adjustments and AUCs from published licensing studies were used to calculate bioavailabilities using the formula: Bioavailability (% of IVIG) = AUC(SCIG) ÷ AUC(IVIG) x 1/Dose Adjustment. We also compared the increment in serum IgG concentration achieved with varying doses of SCIG in recent meta-analyses with the increment with different doses of IVIG, and determined the serum IgG concentrations when patients switched SCIG products at the same dose.
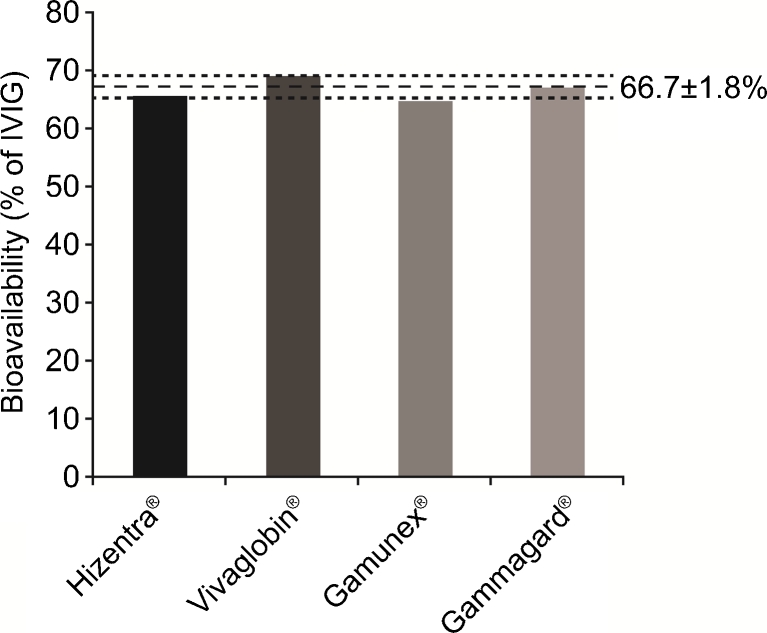
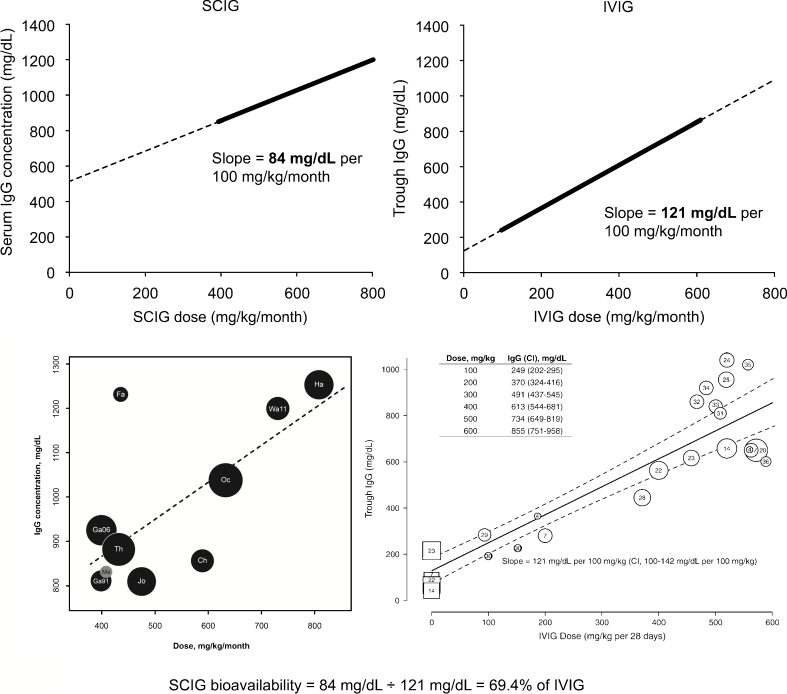
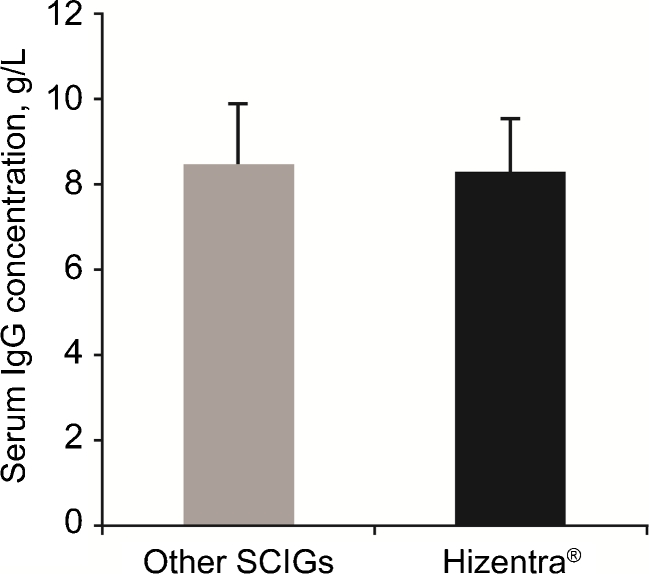
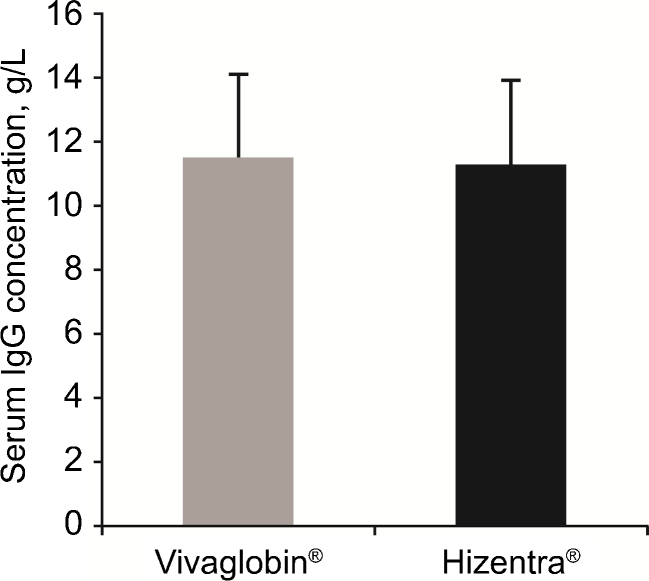
Results: The actual bioavailabilities were: Gamunex® 65.0%, Hizentra® 65.5%, Gammagard® 67.2%, Vivaglobin® 69.0%. Regression analyses of serum IgG vs. dose showed that the mean increase in serum IgG resulting from a 100 mg/kg/month increment in SCIG dosing was 69.4% of the increase with the same increment in IVIG dosing (84 mg/dL vs. 121 mg/dL). Patients switching SCIG preparations at the same dose had no change in serum IgG levels, confirming that bioavailabilities of the SCIG preparations did not differ.
Conclusions: Decreased bioavailability appears to be a basic property of SCIG and not a result of any manufacturing process or concentration. Because serum IgG levels do not vary with different SCIG products at the same dose, adjustments are not necessary when switching products.
Figures
References
-
- Aebersold P. Regulatory requirements for subcutaneous Ig for PID. In: Intravenous immunoglobulins in the 21st century: progress and challenges in efficacy, safety and paths to licensure. FDA workshop. 2005. http://www.fda.gov/downloads/BiologicsBloodVaccines/NewsEvents/Workshops.... Accessed 8 Nov 2012.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
