

Combined use of intraoperative ultrasound and indocyanine green fluorescence imaging to detect liver metastases from colorectal cancer
- PMID: 23458105
- PMCID: PMC3843610
- DOI: 10.1111/hpb.12057
Combined use of intraoperative ultrasound and indocyanine green fluorescence imaging to detect liver metastases from colorectal cancer
Abstract
Objectives: Surgical excision is the standard strategy for managing liver metastases from colorectal carcinoma. The achievement of negative (R0) margins is a major determinant of disease-free survival in these patients. Current imaging techniques are of limited value in achieving this goal. A new approach to the intraoperative detection of colorectal liver metastatic tissue based on the emission of indocyanine green (ICG) fluorescence was evaluated.
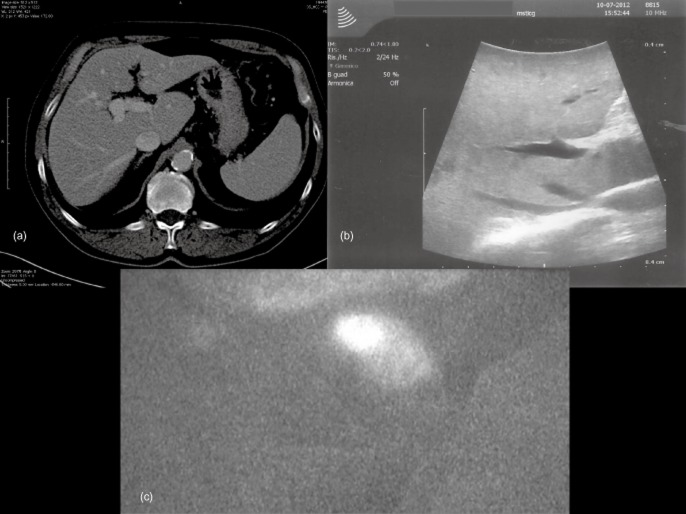
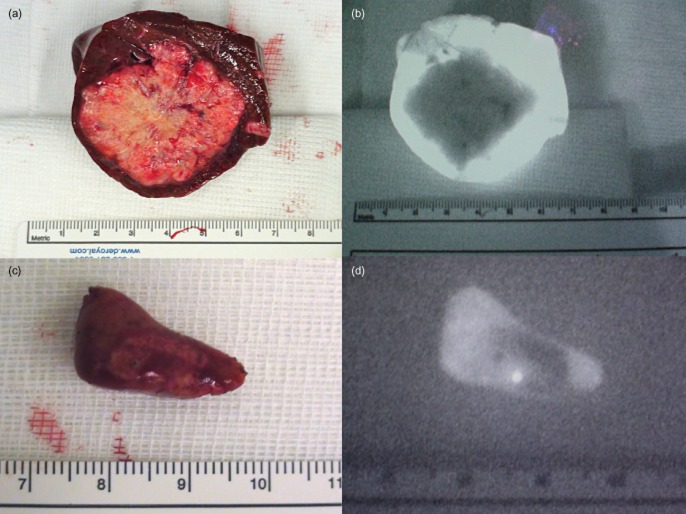
Methods: A total of 25 consecutive patients with liver metastases from primary colorectal cancers who were eligible for liver resection received a bolus of ICG (0.5 mg/kg body weight) 24 h before surgery. During surgery, ICG fluorescence, which accumulates around lesions as a result of defective biliary clearance, was detected with a near-infrared camera system, the Photodynamic Eye (PDE). Numbers of lesions detected by, respectively, PDE + ICG, intraoperative ultrasound (IOUS) and preoperative computed tomography (CT) were recorded.
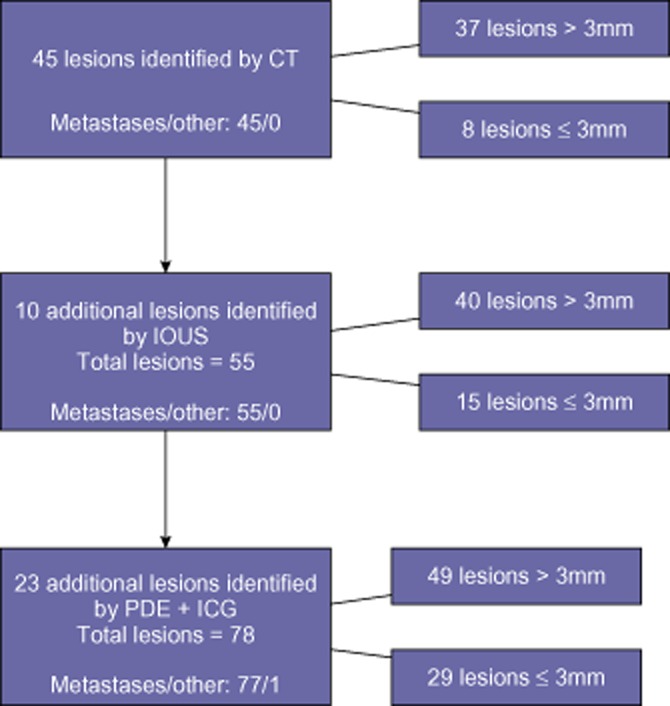
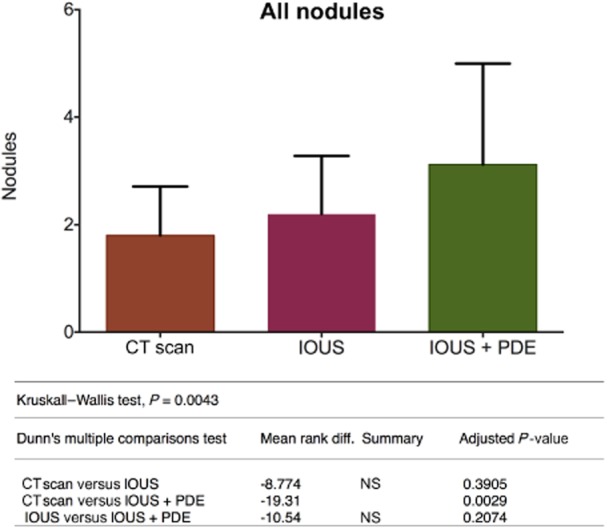
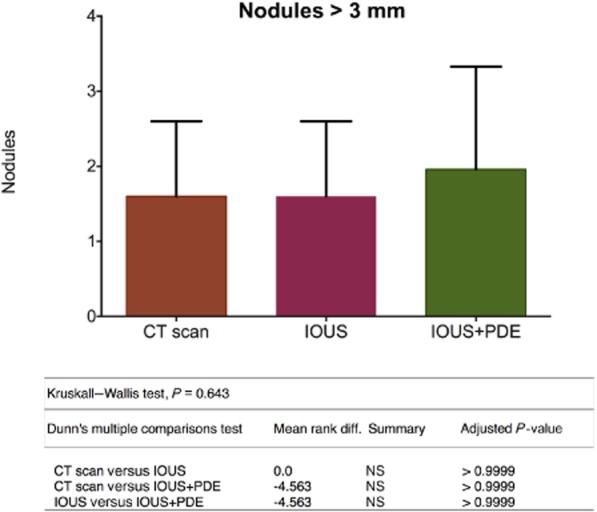
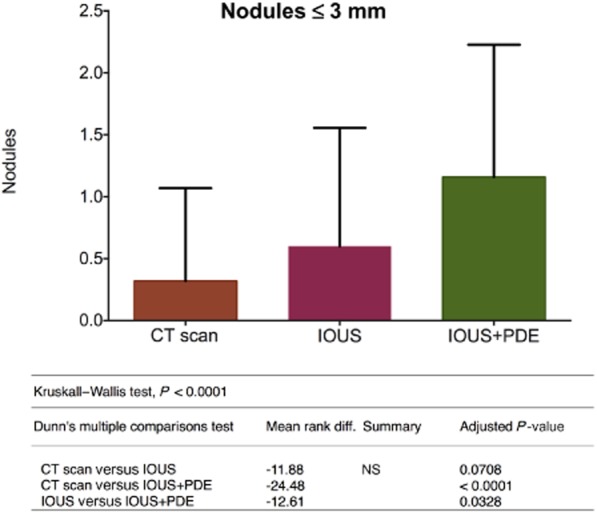
Results: The near-infrared camera plus ICG revealed a total of 77 metastatic liver nodules. Preoperative CT demonstrated 45 (58.4%) and IOUS showed 55 (71.4%). Preoperative CT and IOUS alone were inferior to the combined use of PDE + ICG and IOUS in the detection of lesions of ≤ 3 mm in size.
Conclusions: This experience suggests that PDE + ICG, combined with IOUS, may represent a safe and effective tool for ensuring the complete surgical eradication of liver metastases from colorectal cancer.
© 2013 International Hepato-Pancreato-Biliary Association.
Figures
Similar articles
-
Combined use of contrast-enhanced intraoperative ultrasonography and a fluorescence navigation system for identifying hepatic metastases.World J Surg. 2010 Dec;34(12):2953-9. doi: 10.1007/s00268-010-0764-1. World J Surg. 2010. PMID: 20734045
-
Usefulness of intraoperative diagnosis of hepatic tumors located at the liver surface and hepatic segmental visualization using indocyanine green-photodynamic eye imaging.Eur J Surg Oncol. 2015 Feb;41(2):257-64. doi: 10.1016/j.ejso.2014.09.008. Epub 2014 Oct 18. Eur J Surg Oncol. 2015. PMID: 25447030
-
Perioperative and recurrence-free survival outcomes after laparoscopic hepatectomy for colorectal cancer liver metastases using indocyanine green fluorescence imaging: an inverse probability treatment weighted analysis.Surg Endosc. 2025 Feb;39(2):1169-1181. doi: 10.1007/s00464-024-11478-3. Epub 2024 Dec 23. Surg Endosc. 2025. PMID: 39715956
-
Intraoperative fluorescence imaging with indocyanine green in hepatic resection for malignancy: a systematic review and meta-analysis of diagnostic test accuracy studies.Surg Endosc. 2020 Jul;34(7):2891-2903. doi: 10.1007/s00464-020-07543-2. Epub 2020 Apr 7. Surg Endosc. 2020. PMID: 32266547
-
Intraoperative ultrasound for the colorectal surgeon: current trends and barriers.ANZ J Surg. 2017 Sep;87(9):671-676. doi: 10.1111/ans.14124. Epub 2017 Aug 3. ANZ J Surg. 2017. PMID: 28771975 Review.
Cited by
-
Detection of Colorectal Liver Metastases Using Near-Infrared Fluorescence Imaging During Hepatectomy: Prospective Single Centre UK Study.J Gastrointest Cancer. 2023 Jun;54(2):574-579. doi: 10.1007/s12029-022-00836-w. Epub 2022 May 26. J Gastrointest Cancer. 2023. PMID: 35616823
-
99mTc-68Ga-ICG-Labelled Macroaggregates and Nanocolloids of Human Serum Albumin: Synthesis Procedures of a Trimodal Imaging Agent Using Commercial Kits.Contrast Media Mol Imaging. 2020 Jan 22;2020:3629705. doi: 10.1155/2020/3629705. eCollection 2020. Contrast Media Mol Imaging. 2020. PMID: 32410921 Free PMC article.
-
Application of Fluorescent Dyes in Visceral Surgery: State of the Art and Future Perspectives.Visc Med. 2020 Apr;36(2):80-87. doi: 10.1159/000506910. Epub 2020 Mar 26. Visc Med. 2020. PMID: 32355664 Free PMC article. Review.
-
Intraoperative near infrared functional imaging of rectal cancer using artificial intelligence methods - now and near future state of the art.Eur J Nucl Med Mol Imaging. 2024 Aug;51(10):3135-3148. doi: 10.1007/s00259-024-06731-9. Epub 2024 Jun 11. Eur J Nucl Med Mol Imaging. 2024. PMID: 38858280 Free PMC article. Review.
-
Fluorescence-guided colorectal surgery: applications, clinical results, and protocols.Ann Surg Treat Res. 2023 Nov;105(5):252-263. doi: 10.4174/astr.2023.105.5.252. Epub 2023 Oct 31. Ann Surg Treat Res. 2023. PMID: 38023438 Free PMC article. Review.
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Scheele J, Stangl R, Altendorf-Hofmann A. Hepatic metastases from colorectal carcinoma: impact of surgical resection on the natural history. Br J Surg. 1990;77:1241–1246. - PubMed
-
- Jaffe BM, Donegan WL, Watson F, Spratt JS. Factors influencing survival in patients with untreated hepatic metastases. Surg Gynecol Obstet. 1968;127:1–11. - PubMed
-
- Bengtsson G, Carlsson G, Hafström L, Jönsson PE. Natural history of patients with untreated liver metastases from colorectal cancer. Am J Surg. 1981;141:586–589. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
