

Incidental pT2-T3 gallbladder cancer after a cholecystectomy: outcome of staging at 3 months prior to a radical resection
- PMID: 23458168
- PMCID: PMC3731586
- DOI: 10.1111/hpb.12032
Incidental pT2-T3 gallbladder cancer after a cholecystectomy: outcome of staging at 3 months prior to a radical resection
Abstract
Introduction: Patients with incidental pT2-T3 gallbladder cancer (IGC) after a cholecystectomy may benefit from a radical re-resection although their optimal treatment strategy is not well defined. In this Unit, such patients undergo delayed staging at 3 months after a cholecystectomy to assess the evidence of a residual tumour, extra hepatic spread and the biological behaviour of the tumour. The aim of this study was to evaluate the outcome of patients who had delayed staging at 3 months after a cholecystectomy.
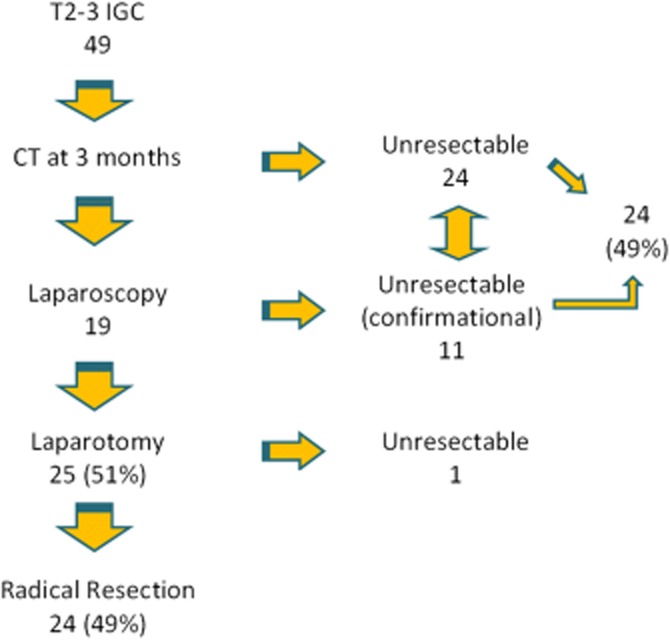
Methods: From July 2003 to July 2011, 56 patients with T2-T3 gallbladder cancer were referred to this Unit of which 49 were diagnosed incidentally on histology after a cholecystectomy. All 49 patients underwent delayed pre-operative staging using multi-detector computed tomography (MDCT) followed selectively by laparoscopy at 3 months after a cholecystectomy. Data were collected from a prospectively held database. The peri-operative and long-term outcomes of patients were analysed. SPSS software was used for statistical analysis.
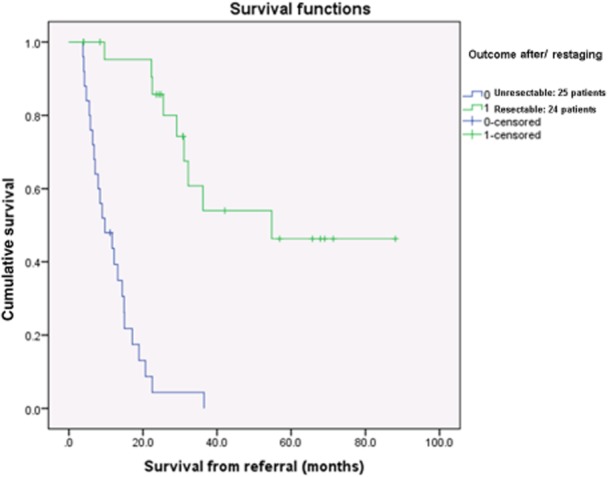
Results: There were 38 pT2 and 11 pT3 tumours. After delayed staging, 24/49 (49%) patients underwent a radical resection, 24/49 (49%) were found to be inoperable on pre-operative assessment and 1/49 (2%) patient underwent an exploratory laparotomy and were found to be unresectable. The overall median survival from referral was 20.7 months (54.8 months for the group who had a radical re-resection versus 9.7 months for the group who had unresectable disease, P < 0.001). These results compare favourably with the reported outcome of fast-track management for incidental pT2-T3 gallbladder cancer from other major series in the literature.
Conclusion: Delayed staging in patients with incidental T2-T3 gallbladder cancer after a cholecystectomy is a useful strategy to select patients who will benefit from a resection and avoid unnecessary major surgery.
© 2013 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Goetze TO, Paolucci V. Adequate extent in radical re-resection of incidental gallbladder carcinoma: analysis of the German Registry. Surg Endosc. 2010;24:2156–2164. - PubMed
-
- American College of Surgeons/American Cancer Society National Cancer Data Base, based on more than 10,000 patients diagnosed with gallbladder cancer from 1989 to 1996. (Apr 2012.) http://www.cancer.org/acs/groups/cid/documents/webcontent/003101-pdf.pdf (last accessed 12 December 2012)
-
- Hueman MT, Vollmer CM, Jr, Pawlik TM. Evolving treatment strategies for gallbladder cancer. Ann Surg Oncol. 2009;16:2101–2115. - PubMed
-
- Glauser PM, Strub D, Kaser SA, Mattiello D, Rieben F, Maurer CA. Incidence, management, and outcome of incidental gallbladder carcinoma: analysis of the database of the Swiss association of laparoscopic and thoracoscopic surgery. Surg Endosc. 2010;24:2281–2286. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
