

Evaluation of stapler hepatectomy during a laparoscopic liver resection
- PMID: 23458439
- PMCID: PMC4503281
- DOI: 10.1111/hpb.12043
Evaluation of stapler hepatectomy during a laparoscopic liver resection
Abstract
Methods: An international database of 1499 laparoscopic liver resections was analysed using multivariate and Kaplan-Meier analysis.
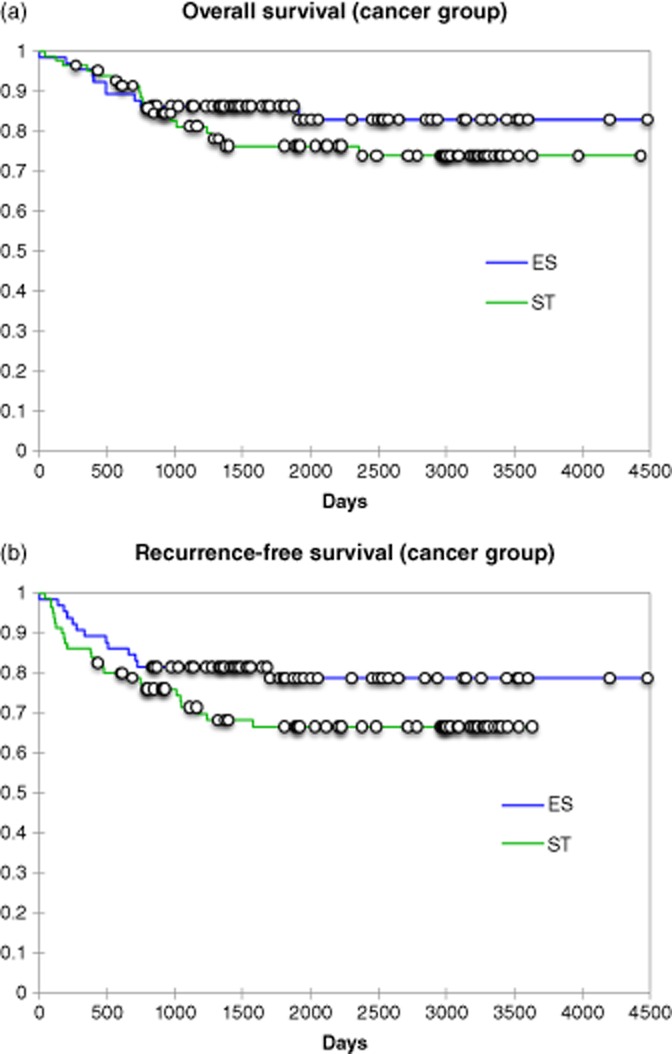
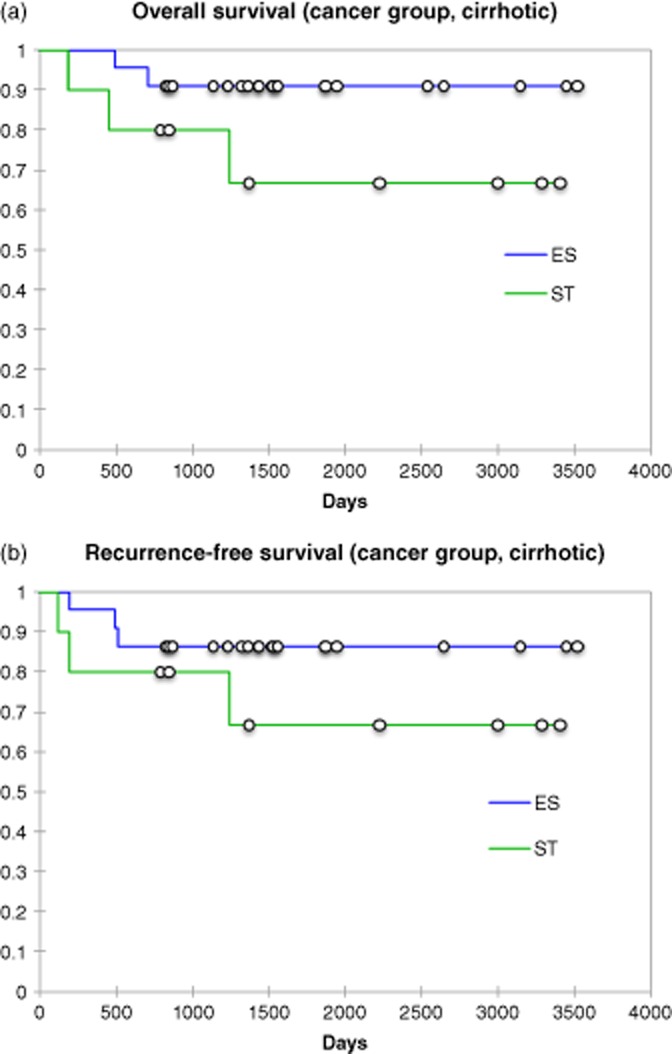
Results: In total, 764 stapler hepatectomies (SH) were compared with 735 electrosurgical resections (ER). SH was employed in larger tumours (4.5 versus 3.8 cm; P < 0.003) with decreased operative times (2.6 versus 3.1 h; P < 0.001), blood loss (100 versus 200 cc; P < 0.001) and length of stay (3.0 versus 7.0 days; P < 0.001). SH incurred a trend towards higher complications (16% versus 13%; P = 0.057) including bile leaks (26/764, 3.4% versus 16/735, 2.2%: P = 0.091). To address group homogeneity, a subset analysis of lobar resections confirmed the benefits of SH. Kaplan-Meier analysis in non-cirrhotic and cirrhotic patients confirmed equivalent patient (P = 0.290 and 0.118) and disease-free survival (P = 0.120 and 0.268). Multivariate analysis confirmed the parenchymal transection technique did not increase the risk of cancer recurrence, whereas tumour size, the presence of cirrhosis and concomitant operations did.
Conclusions: A SH provides several advantages including: diminished blood loss, transfusion requirements and shorter operative times. In spite of the smaller surgical margins in the SH group, equivalent recurrence and survival rates were observed when matched for parenchyma and extent of resection.
© 2013 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Lefor AT, Flowers JL. Laparoscopic wedge biopsy of the liver. J Am Coll Surg. 1994;178:307–308. - PubMed
-
- Lefor AT, Flowers JL, Heyman MR. Laparoscopic staging of Hodgkin's disease. Surg Oncol. 1993;2:217–220. - PubMed
-
- Fong Y, Blumgart LH. Useful stapling techniques in liver surgery. J Am Coll Surg. 1997;185:93–100. - PubMed
-
- McEntee GP, Nagorney DM. Use of vascular staplers in major hepatic resections. Br J Surg. 1991;78:40–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
