

Effects of introducing an enhanced recovery after surgery programme for patients undergoing open hepatic resection
- PMID: 23458488
- PMCID: PMC3608984
- DOI: 10.1111/j.1477-2574.2012.00578.x
Effects of introducing an enhanced recovery after surgery programme for patients undergoing open hepatic resection
Abstract
Objectives: Enhanced recovery after surgery (ERAS) protocols are coming to represent the standard of care in many surgical procedures, yet data on their use following hepatic surgery are scarce. The aim of this study was to review outcomes after the introduction of an ERAS programme for patients undergoing open hepatic resection.
Methods: A retrospective review of patients undergoing open hepatic resection from March 2005 to June 2011 was carried out. The primary outcome measure was total hospital length of stay (LoS) (including readmissions). Principles associated with enhanced recovery after surgery were documented and analysed as independent predictors of hospital LoS.
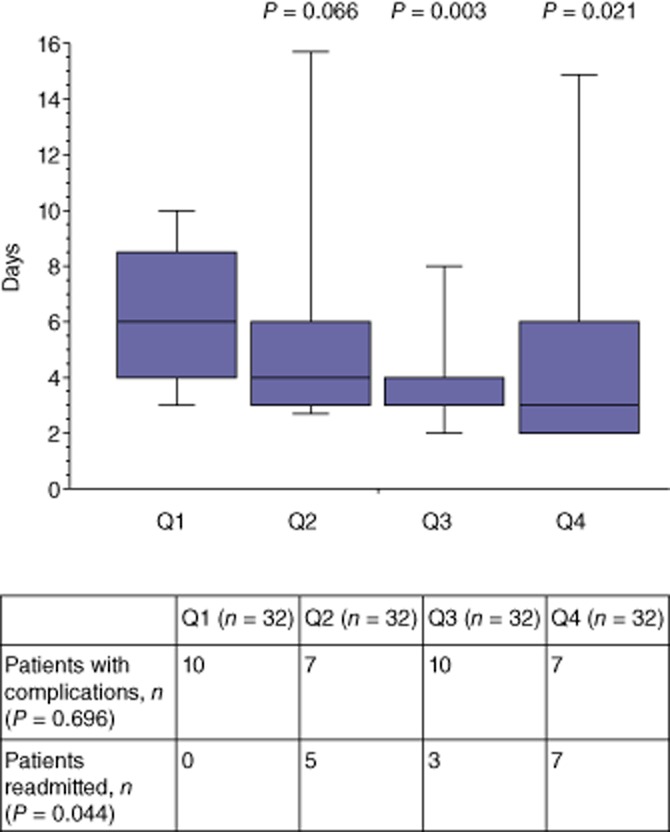
Results: A total of 120 patients underwent 128 consecutive hepatic resections, 84 (65.6%) of which were performed in patients with underlying colorectal metastases and 64 (50.0%) of which comprised major hepatic resections. The median hospital LoS was reduced from 6 days to 3 days from the first to the fourth quartiles of the study population (P = 0.021). The proportion of patients suffering complications (26.6%) remained constant across the series. Readmissions increased from the first quartile (none of 32 patients) to the fourth quartile (seven of 32 patients) (P = 0.044). Following multivariate analysis, only the development of a complication (P < 0.001), total postoperative i.v. fluid (P = 0.003) and formation of an anastomosis (P = 0.006) were independent predictors of hospital LoS.
Conclusions: An ERAS programme can be successfully applied to patients undergoing open hepatic resection with a reduction in hospital LoS, but an increase in the rate of readmissions.
© 2012 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Lassen K, Soop M, Nygren J, Cox PB, Hendry PO, Spies C, et al. Consensus review of optimal perioperative care in colorectal surgery: ERAS group recommendations. Arch Surg. 2009;144:961–969. - PubMed
-
- Gouvas N, Tan E, Windsor A, Xynos E, Tekkis PP. Fast-track vs. standard care in colorectal surgery: a meta-analysis update. Int J Colorectal Dis. 2009;24:1119–1131. - PubMed
-
- van Dam RM, Hendry PO, Coolsen MM, Bemelmans MH, Lassen K, Revhag A, et al. Initial experience with a multi-modal enhanced recovery programme in patients undergoing liver resection. Br J Surg. 2008;95:969–975. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
