

Chronic neuropathologies of single and repetitive TBI: substrates of dementia?
- PMID: 23458973
- PMCID: PMC4513655
- DOI: 10.1038/nrneurol.2013.29
Chronic neuropathologies of single and repetitive TBI: substrates of dementia?
Abstract
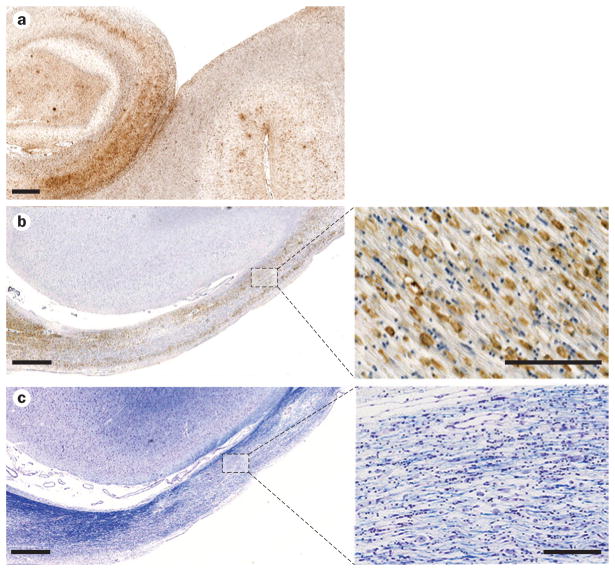
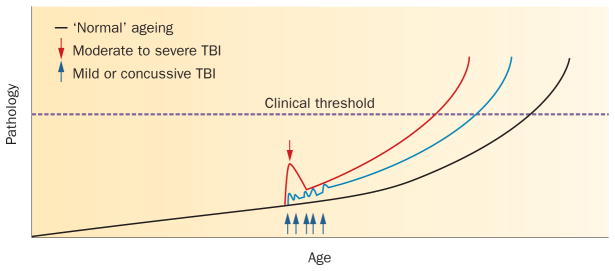
Traumatic brain injury (TBI) has long been recognized to be a risk factor for dementia. This association has, however, only recently gained widespread attention through the increased awareness of 'chronic traumatic encephalopathy' (CTE) in athletes exposed to repetitive head injury. Originally termed 'dementia pugilistica' and linked to a career in boxing, descriptions of the neuropathological features of CTE include brain atrophy, cavum septum pellucidum, and amyloid-β, tau and TDP-43 pathologies, many of which might contribute to clinical syndromes of cognitive impairment. Similar chronic pathologies are also commonly found years after just a single moderate to severe TBI. However, little consensus currently exists on specific features of these post-TBI syndromes that might permit their confident clinical and/or pathological diagnosis. Moreover, the mechanisms contributing to neurodegeneration following TBI largely remain unknown. Here, we review the current literature and controversies in the study of chronic neuropathological changes after TBI.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Molgaard CA, et al. Epidemiology of head trauma and neurocognitive impairment in a multi-ethnic population. Neuroepidemiology. 1990;9:233–242. - PubMed
-
- Mortimer JA, French LR, Hutton JT, Schuman LM. Head injury as a risk factor for Alzheimer’s disease. Neurology. 1985;35:264–267. - PubMed
-
- Mortimer JA, et al. Head trauma as a risk factor for Alzheimer’s disease: a collaborative re-analysis of case–control studies. EURODEM Risk Factors Research Group. Int J Epidemiol. 1991;20 (Suppl 2):S28–S35. - PubMed
-
- Graves AB, et al. The association between head trauma and Alzheimer’s disease. Am J Epidemiol. 1990;131:491–501. - PubMed
-
- O’Meara ES, et al. Head injury and risk of Alzheimer’s disease by apolipoprotein E genotype. Am J Epidemiol. 1997;146:373–384. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
