

Placental histopathological changes associated with Plasmodium vivax infection during pregnancy
- PMID: 23459254
- PMCID: PMC3573078
- DOI: 10.1371/journal.pntd.0002071
Placental histopathological changes associated with Plasmodium vivax infection during pregnancy
Erratum in
- PLoS Negl Trop Dis. 2013 Apr;7(4). doi: 10.1371/annotation/28901e80-13ad-4cae-99e8-8d54625743b6. Epiphânio, Sabrina [corrected to Epiphanio, Sabrina]
Abstract
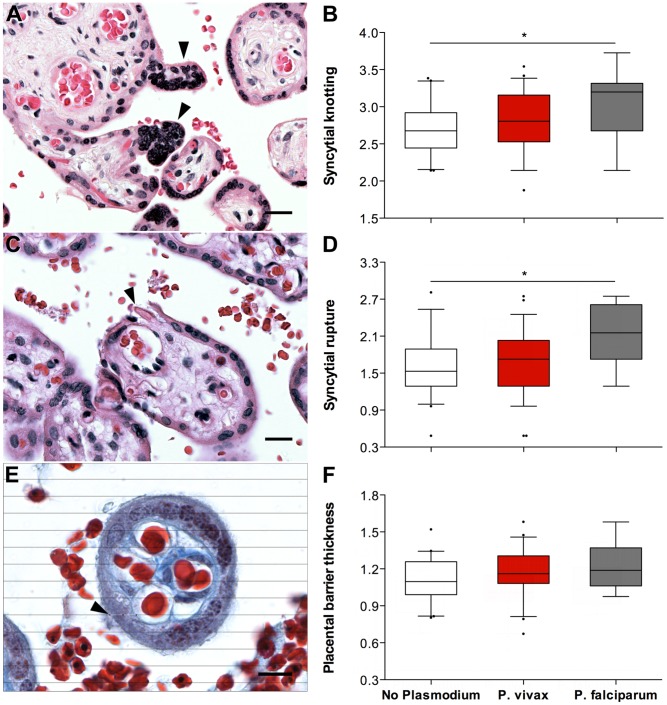
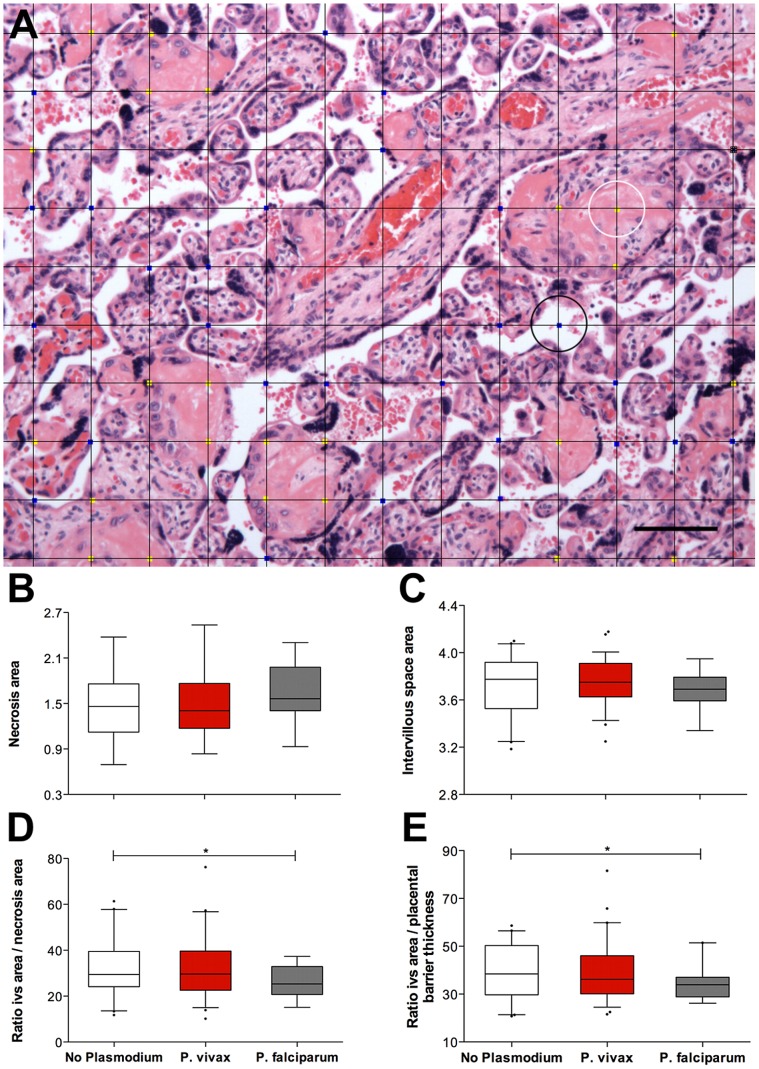
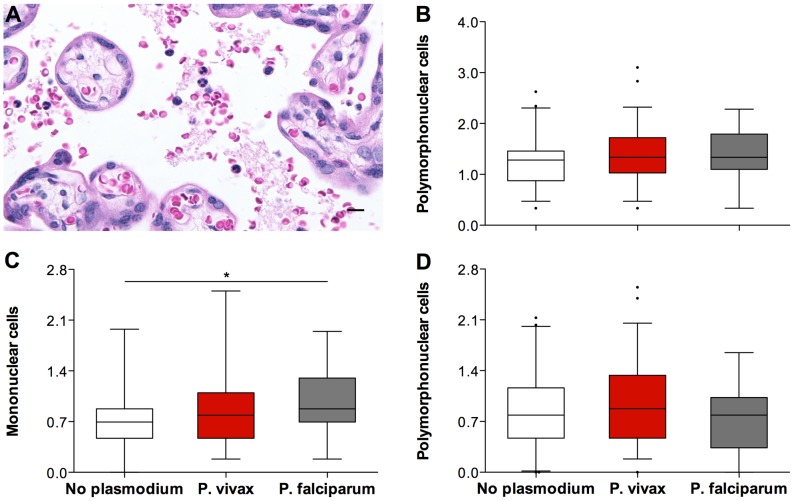
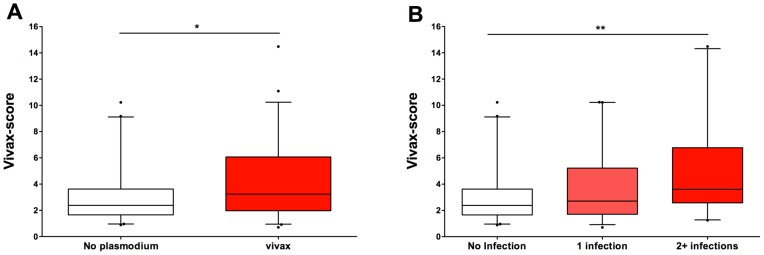
Histological evidence of Plasmodium in the placenta is indicative of placental malaria, a condition associated with severe outcomes for mother and child. Histological lesions found in placentas from Plasmodium-exposed women include syncytial knotting, syncytial rupture, thickening of the placental barrier, necrosis of villous tissue and intervillositis. These histological changes have been associated with P. falciparum infections, but little is known about the contribution of P. vivax to such changes. We conducted a cross-sectional study with pregnant women at delivery and assigned them to three groups according to their Plasmodium exposure during pregnancy: no Plasmodium exposure (n = 41), P. vivax exposure (n = 59) or P. falciparum exposure (n = 19). We evaluated their placentas for signs of Plasmodium and placental lesions using ten histological parameters: syncytial knotting, syncytial rupture, placental barrier thickness, villi necrosis, intervillous space area, intervillous leucocytes, intervillous mononucleates, intervillous polymorphonucleates, parasitized erythrocytes and hemozoin. Placentas from P. vivax-exposed women showed little evidence of Plasmodium or hemozoin but still exhibited more lesions than placentas from women not exposed to Plasmodium, especially when infections occurred twice or more during pregnancy. In the Brazilian state of Acre, where diagnosis and primary treatment are readily available and placental lesions occur in the absence of detected placental parasites, relying on the presence of Plasmodium in the placenta to evaluate Plasmodium-induced placental pathology is not feasible. Multivariate logistic analysis revealed that syncytial knotting (odds ratio [OR], 4.21, P = 0.045), placental barrier thickness (OR, 25.59, P = 0.021) and mononuclear cells (OR, 4.02, P = 0.046) were increased in placentas from P. vivax-exposed women when compared to women not exposed to Plasmodium during pregnancy. A vivax-score was developed using these three parameters (and not evidence of Plasmodium) that differentiates between placentas from P. vivax-exposed and unexposed women. This score illustrates the importance of adequate management of P. vivax malaria during pregnancy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Steketee RW, Nahlen BL, Parise ME, Menendez C (2001) The burden of malaria in pregnancy in malaria-endemic areas. The American journal of tropical medicine and hygiene 64: 28–35. - PubMed
-
- Rogerson SJ, Hviid L, Duffy PE, Leke RF, Taylor DW (2007) Malaria in pregnancy: pathogenesis and immunity. Lancet Infect Dis 7: 105–117. - PubMed
-
- Menendez C (2006) Malaria during pregnancy. Current Molecular Medicine 6: 269–273. - PubMed
-
- Nosten F, McGready R, Simpson JA, Thwai KL, Balkan S, et al. (1999) Effects of Plasmodium vivax malaria in pregnancy. Lancet 354: 546–549. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
