

Adenoid cystic carcinoma: clinical and molecular features
- PMID: 23463073
- PMCID: PMC3597152
- DOI: 10.1007/s12105-013-0426-3
Adenoid cystic carcinoma: clinical and molecular features
Abstract
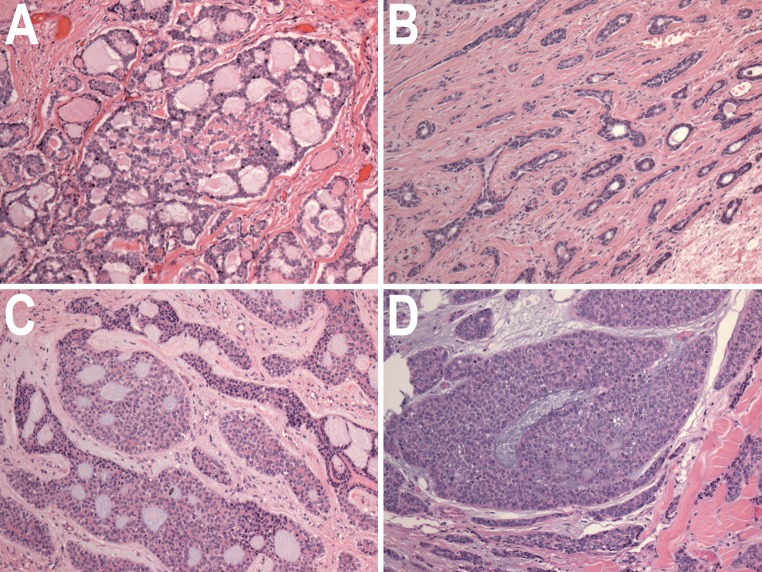
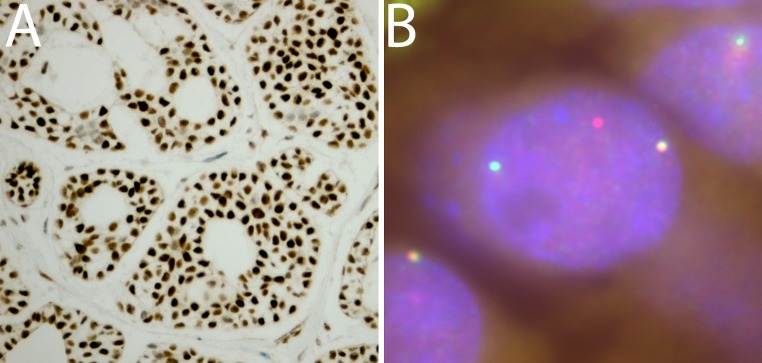
The clinical features and common molecular alterations of adenoid cystic carcinoma (ACC) are reviewed in this paper. ACC is an uncommon neoplasm that most frequently arises in salivary glands and related tissue in the head and neck region. ACC has distinct histologic features, with cribriform and tubular growth patterns of basaloid cells displaying a predominantly myoepithelial cellular phenotype. This neoplasm also has uncommon clinical features of rare regional lymph node metastasis and a prolonged but relentlessly progressive clinical course. Clinical outcome in ACC is correlated to histologic grade, which is correlated to the degree of aneuploidy and genetic alterations present in the tumor genomes. Recent studies have identified that the majority of ACC contain alterations of the MYB gene, usually resulting in a fusion gene product with the NFIB gene by a t(6;9) translocation event. The molecular consequences of this alteration are incompletely understood, as are secondary molecular alterations that contribute to the neoplastic phenotype of ACC.
Figures
References
-
- Bonaparte JP, Hart R, Trites J, Taylor MS. Incidence of adenoid cystic carcinoma in nova scotia: 30-year population-based epidemiologic study. J Otolaryngol Head Neck Surg. 2008;37:642–648. - PubMed
-
- Vander Poorten VL, Balm AJ, Hilgers FJ, Tan IB, Loftus-Coll BM, Keus RB, Hart AA. Prognostic factors for long term results of the treatment of patients with malignant submandibular gland tumors. Cancer. 1999;85:2255–2264. doi: 10.1002/(SICI)1097-0142(19990515)85:10<2255::AID-CNCR22>3.0.CO;2-D. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
