

Quantitative video-oculography to help diagnose stroke in acute vertigo and dizziness: toward an ECG for the eyes
- PMID: 23463752
- PMCID: PMC8448203
- DOI: 10.1161/STROKEAHA.111.000033
Quantitative video-oculography to help diagnose stroke in acute vertigo and dizziness: toward an ECG for the eyes
Abstract
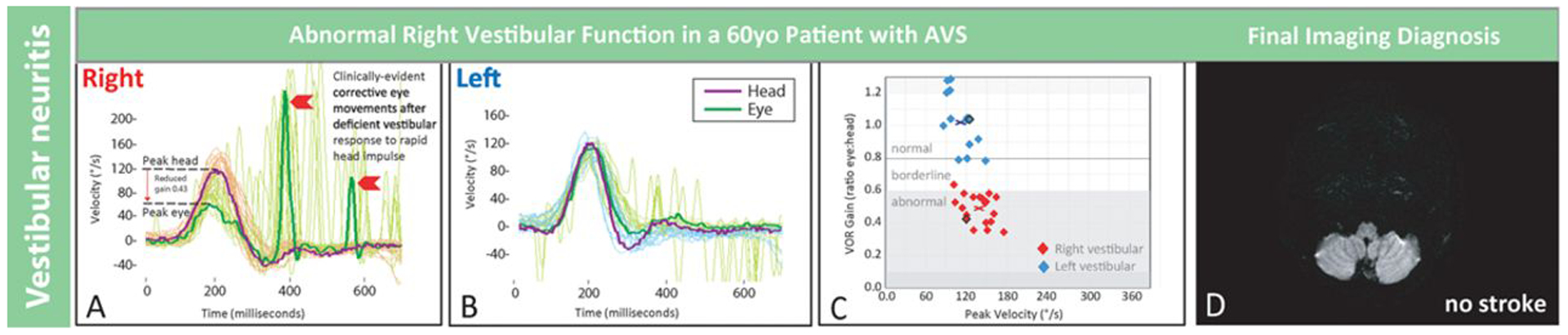
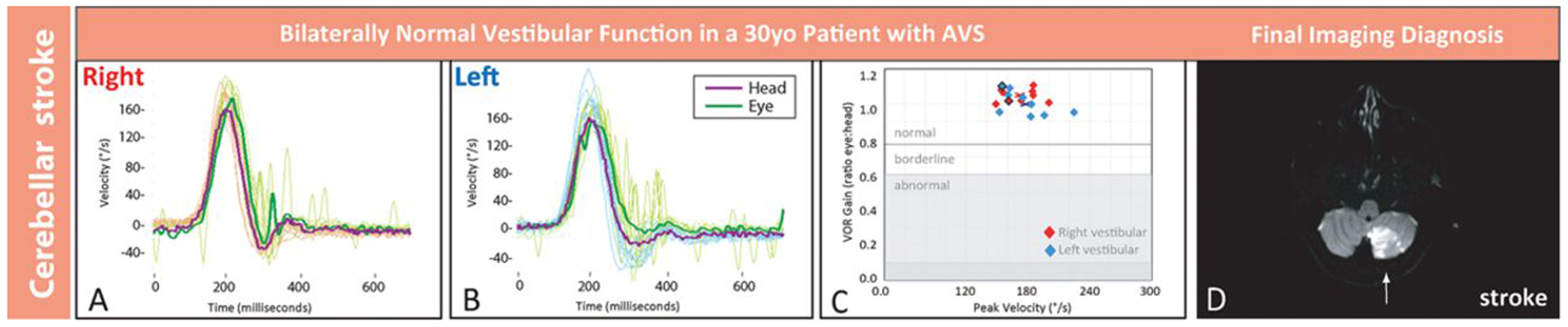
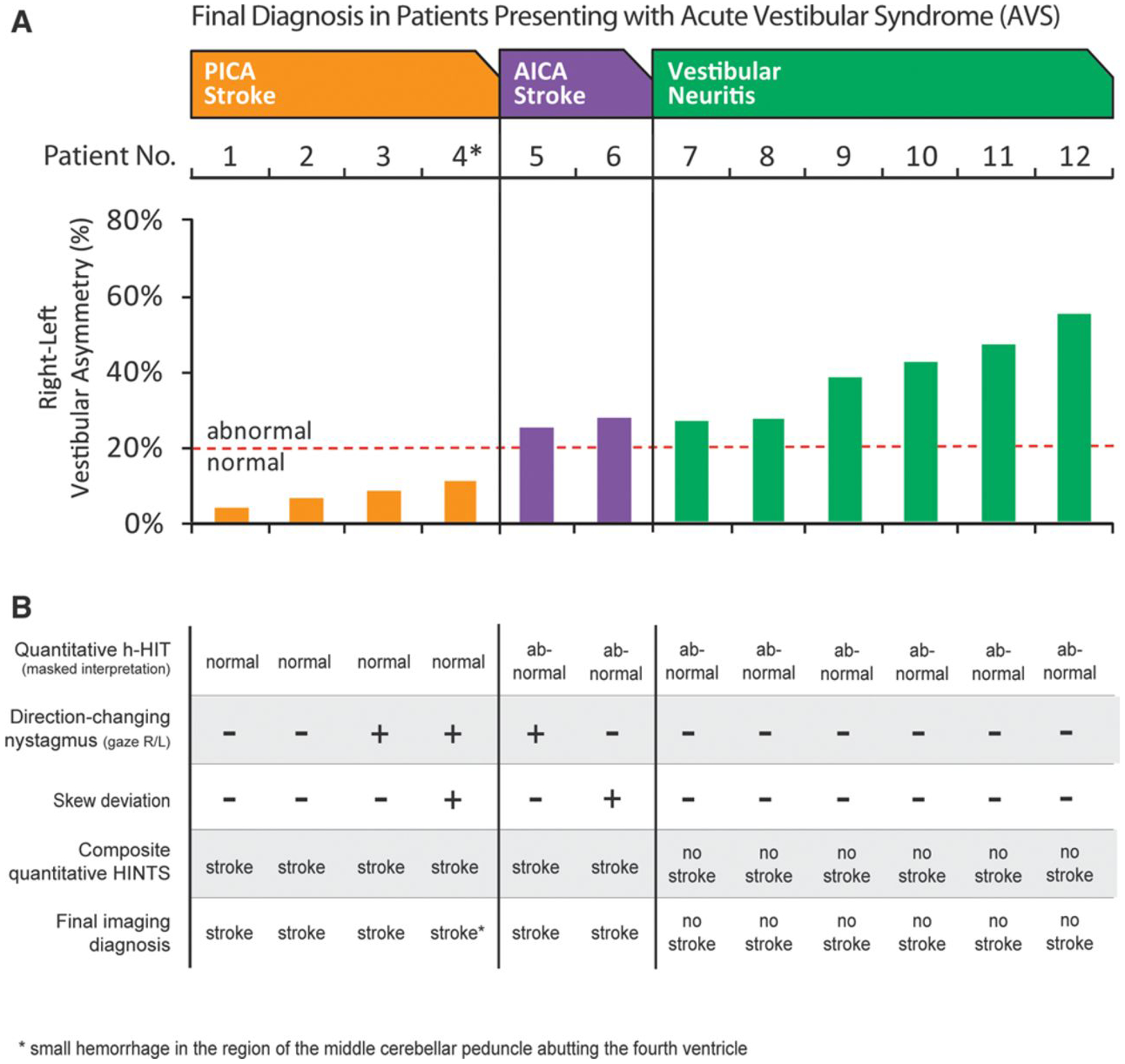
Background and purpose: Strokes can be distinguished from benign peripheral causes of acute vestibular syndrome using bedside oculomotor tests (head impulse test, nystagmus, test-of-skew). Using head impulse test, nystagmus, test-of-skew is more sensitive and less costly than early magnetic resonance imaging for stroke diagnosis in acute vestibular syndrome but requires expertise not routinely available in emergency departments. We sought to begin standardizing the head impulse test, nystagmus, test-of-skew diagnostic approach for eventual emergency department use through the novel application of a portable video-oculography device measuring vestibular physiology in real time. This approach is conceptually similar to ECG to diagnose acute cardiac ischemia.
Methods: Proof-of-concept study (August 2011 to June 2012). We recruited adult emergency department patients with acute vestibular syndrome defined as new, persistent vertigo/dizziness, nystagmus, and (1) nausea/vomiting, (2) head motion intolerance, or (3) new gait unsteadiness. We recorded eye movements, including quantitative horizontal head impulse testing of vestibulo-ocular-reflex function. Two masked vestibular experts rated vestibular findings, which were compared with final radiographic gold-standard diagnoses. Masked neuroimaging raters determined stroke or no stroke using magnetic resonance imaging of the brain with diffusion-weighted imaging obtained 48 hours to 7 days after symptom onset.
Results: We enrolled 12 consecutive patients who underwent confirmatory magnetic resonance imaging. Mean age was 61 years (range 30-73), and 10 were men. Expert-rated video-oculography-based head impulse test, nystagmus, test-of-skew examination was 100% accurate (6 strokes, 6 peripheral vestibular).
Conclusions: Device-based physiological diagnosis of vertebrobasilar stroke in acute vestibular syndrome should soon be possible. If confirmed in a larger sample, this bedside eye ECG approach could eventually help fulfill a critical need for timely, accurate, efficient diagnosis in emergency department patients with vertigo or dizziness who are at high risk for stroke.
Figures
References
-
- Newman-Toker DE, Kattah JC, Alvernia JE, Wang DZ. Normal head impulse test differentiates acute cerebellar strokes from vestibular neuritis. Neurology. 2008;70(24 pt 2):2378–2385. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
