

Cost-effective diagnostic checklists for meningitis in resource-limited settings
- PMID: 23466647
- PMCID: PMC3683123
- DOI: 10.1097/QAI.0b013e31828e1e56
Cost-effective diagnostic checklists for meningitis in resource-limited settings
Abstract
Background: Checklists can standardize patient care, reduce errors, and improve health outcomes. For meningitis in resource-limited settings, with high patient loads and limited financial resources, central nervous system diagnostic algorithms may be useful to guide diagnosis and treatment. However, the cost effectiveness of such algorithms is unknown.
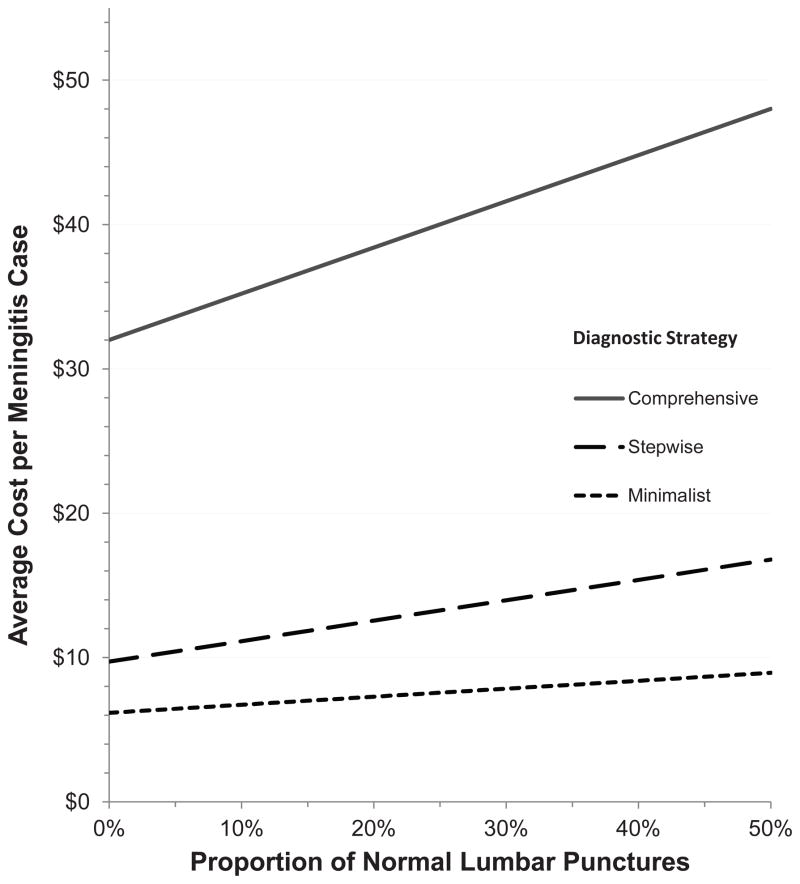
Methods: We used decision analysis methodology to evaluate the costs, diagnostic yield, and cost effectiveness of diagnostic strategies for adults with suspected meningitis in resource-limited settings with moderate/high HIV prevalence. We considered 3 strategies: (1) comprehensive "shotgun" approach of utilizing all routine tests; (2) "stepwise" strategy with tests performed in a specific order with additional tuberculosis (TB) diagnostics; (3) "minimalist" strategy of sequential ordering of high-yield tests only. Each strategy resulted in 1 of 4 meningitis diagnoses: bacterial (4%), cryptococcal (59%), TB (8%), or other (aseptic) meningitis (29%). In model development, we utilized prevalence data from 2 Ugandan sites and published data on test performance. We validated the strategies with data from Malawi, South Africa, and Zimbabwe.
Results: The current comprehensive testing strategy resulted in 93.3% correct meningitis diagnoses costing $32.00 per patient. A stepwise strategy had 93.8% correct diagnoses costing an average of $9.72 per patient, and a minimalist strategy had 91.1% correct diagnoses costing an average of $6.17 per patient. The incremental cost-effectiveness ratio was $133 per additional correct diagnosis for the stepwise over minimalist strategy.
Conclusions: Through strategically choosing the order and type of testing coupled with disease prevalence rates, algorithms can deliver more care more efficiently. The algorithms presented herein are generalizable to East Africa and Southern Africa.
Conflict of interest statement
Figures
References
-
- Somand D, Meurer W. Central nervous system infections. Emerg Med Clin North Am. 2009;27(1):89–100. ix. - PubMed
-
- Trachtenberg JD, Kambugu AD, McKellar M, et al. The medical management of central nervous system infections in Uganda and the potential impact of an algorithm-based approach to improve outcomes. Int J Infect Dis. 2007;11(6):524–530. - PubMed
-
- WHO. [Accessed 15 April 2012.];Towards Universal Access: Scaling up priority HIV/AIDS interventions in the health sector 2010. 2010 Available at: http://www.who.int/hiv/pub/2010progressreport/full_report_en.pdf.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
