

Roux-en-Y versus Billroth I reconstruction after distal gastrectomy for gastric cancer: a meta-analysis
- PMID: 23467403
- PMCID: PMC3582002
- DOI: 10.3748/wjg.v19.i7.1124
Roux-en-Y versus Billroth I reconstruction after distal gastrectomy for gastric cancer: a meta-analysis
Abstract
Aim: To conduct a meta-analysis to compare Roux-en-Y (R-Y) gastrojejunostomy with gastroduodenal Billroth I (B-I) anastomosis after distal gastrectomy (DG) for gastric cancer.
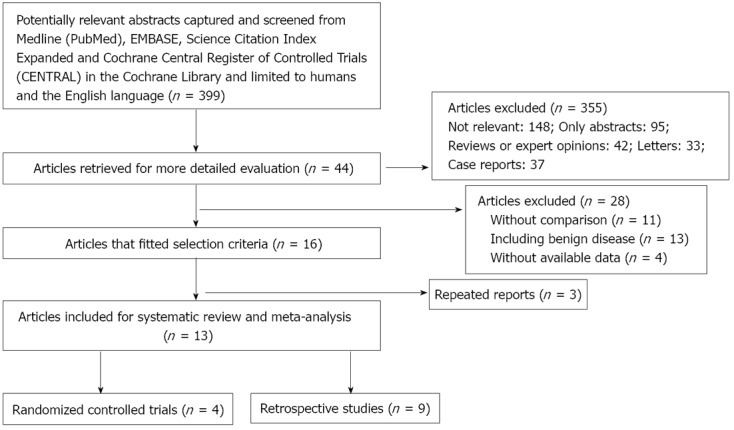
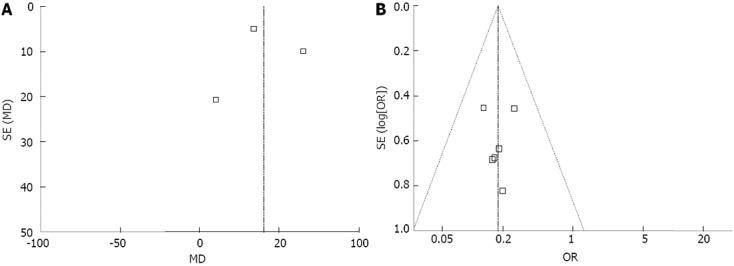
Methods: A literature search was performed to identify studies comparing R-Y with B-I after DG for gastric cancer from January 1990 to November 2012 in Medline, Embase, Science Citation Index Expanded and the Cochrane Central Register of Controlled Trials in The Cochrane Library. Pooled odds ratios (OR) or weighted mean differences (WMD) with 95%CI were calculated using either fixed or random effects model. Operative outcomes such as operation time, intraoperative blood loss and postoperative outcomes such as anastomotic leakage and stricture, bile reflux, remnant gastritis, reflux esophagitis, dumping symptoms, delayed gastric emptying and hospital stay were the main outcomes assessed. Meta-analyses were performed using RevMan 5.0 software (Cochrane library).
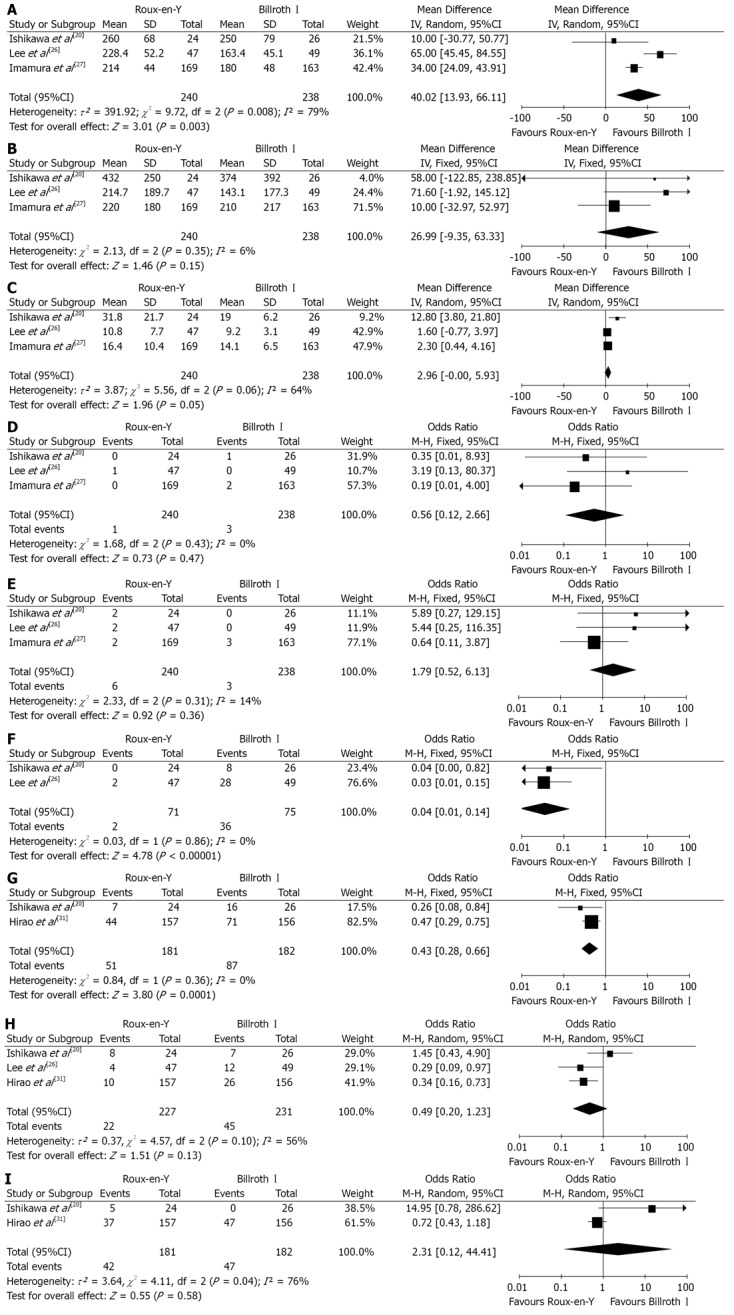
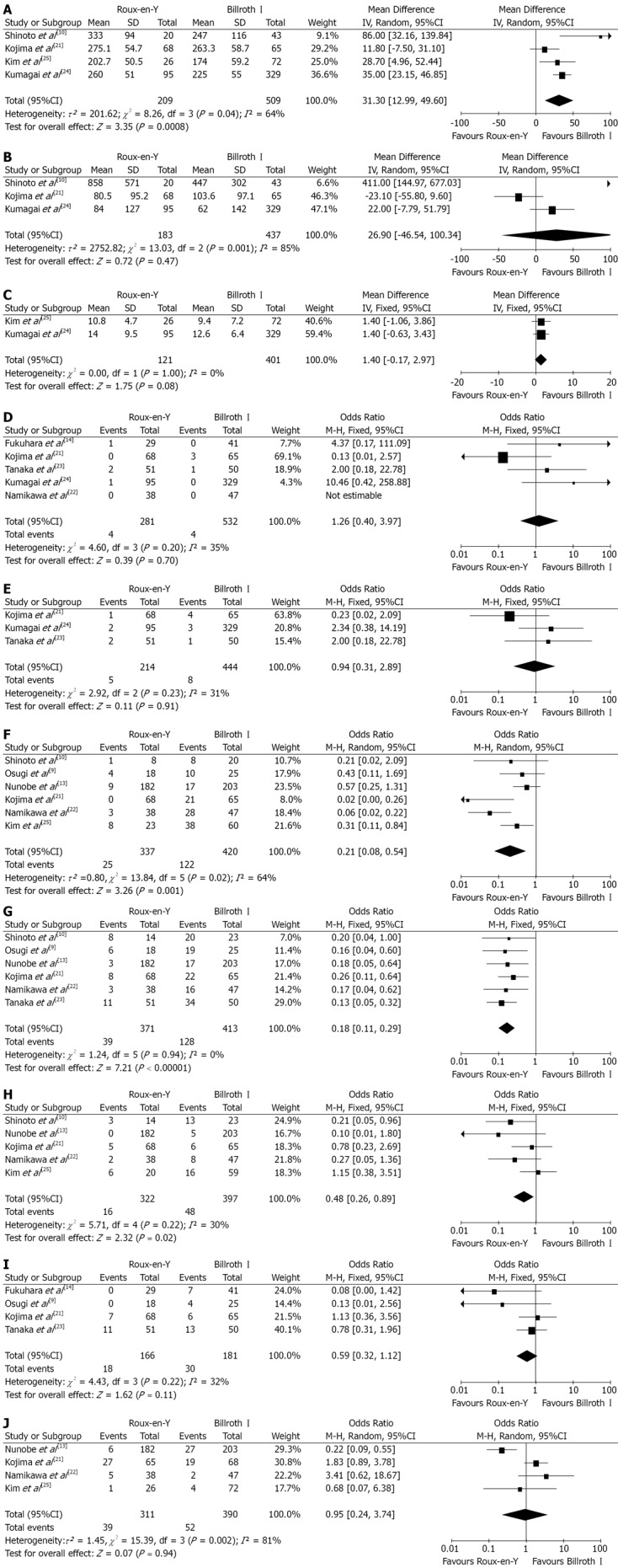
Results: Four randomized controlled trials (RCTs) and 9 non-randomized observational clinical studies (OCS) involving 478 and 1402 patients respectively were included. Meta-analysis of RCTs revealed that R-Y reconstruction was associated with a reduced bile reflux (OR 0.04, 95%CI: 0.01, 0.14; P < 0.00 001) and remnant gastritis (OR 0.43, 95%CI: 0.28, 0.66; P = 0.0001), however needing a longer operation time (WMD 40.02, 95%CI: 13.93, 66.11; P = 0.003). Meta-analysis of OCS also revealed R-Y reconstruction had a lower incidence of bile reflux (OR 0.21, 95%CI: 0.08, 0.54; P = 0.001), remnant gastritis (OR 0.18, 95%CI: 0.11, 0.29; P < 0.00 001) and reflux esophagitis (OR 0.48, 95%CI: 0.26, 0.89; P = 0.02). However, this reconstruction method was found to be associated with a longer operation time (WMD 31.30, 95%CI: 12.99, 49.60; P = 0.0008).
Conclusion: This systematic review point towards some clinical advantages that are rendered by R-Y compared to B-I reconstruction post DG. However there is a need for further adequately powered, well-designed RCTs comparing the same.
Keywords: Billroth I; Distal gastrectomy; Gastric cancer; Meta-analysis; Reconstruction; Roux-en-Y.
Figures
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Kim JP. Current status of surgical treatment of gastric cancer. J Surg Oncol. 2002;79:79–80. - PubMed
-
- Roukos DH. Current advances and changes in treatment strategy may improve survival and quality of life in patients with potentially curable gastric cancer. Ann Surg Oncol. 1999;6:46–56. - PubMed
-
- Nakajima T. Gastric cancer treatment guidelines in Japan. Gastric Cancer. 2002;5:1–5. - PubMed
-
- Yoshino K. [History of gastric cancer surgery] Nihon Geka Gakkai Zasshi. 2000;101:855–860. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
