

Fear-learning deficits in subjects with fibromyalgia syndrome?
- PMID: 23468076
- PMCID: PMC3929307
- DOI: 10.1002/j.1532-2149.2013.00300.x
Fear-learning deficits in subjects with fibromyalgia syndrome?
Abstract
Background: Fibromyalgia syndrome (FMS) is frequently associated with psychiatric conditions, particularly anxiety. Deficits in contingency learning during fear conditioning have been hypothesized to increase anxiety and, consequently, pain sensation in susceptible individuals. The goal of this study was to examine the relationship between contingency learning and pain experience in subjects with FMS and rheumatoid arthritis (RA).
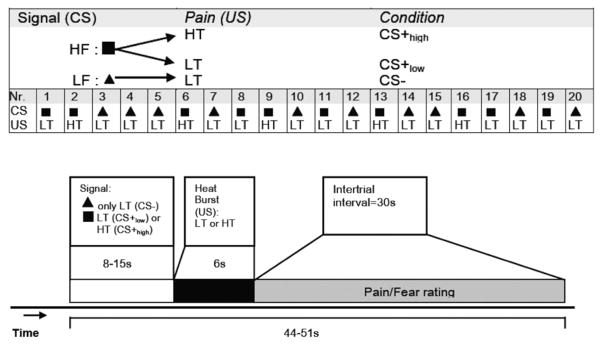
Methods: Fourteen female FMS subjects, 14 age-matched female RA subjects and 14 age-matched female healthy controls (HCs) were included in a fear-conditioning experiment. The conditioned stimulus (CS) consisted of visual signs, the unconditioned stimulus (US) of thermal stimuli. CS- predicted low-temperature exposure (US), while CS+ was followed by low or high temperature.
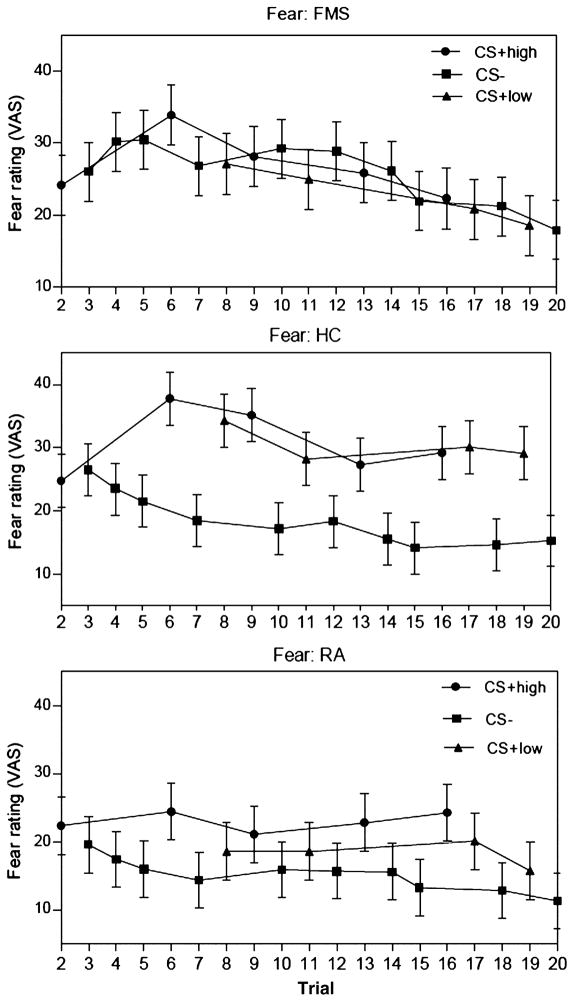
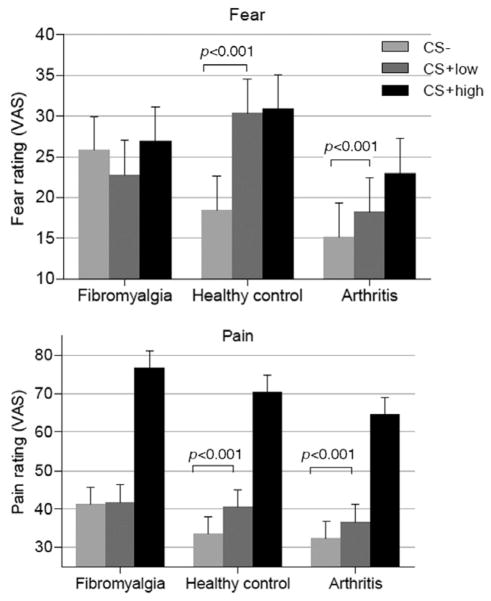
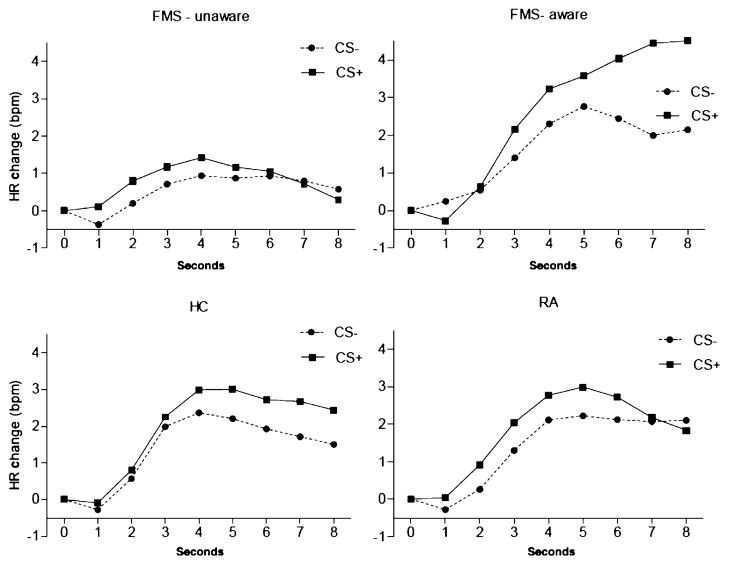
Results: In the FMS group, only 50% of the subjects were aware of the US-CS contingency, whereas 86% of the RA subjects and all of the HCs were aware of the contingency. CS+ induced more anxiety than CS- in RA subjects and HCs. As expected, low-temperature exposure was experienced as less painful after CS- than after CS+ in these subjects. FMS subjects did not show such adaptive conditioning. The effects of the type of CS on heart rate changes were significant in the HCs and the aware FMS subjects, but not in the unaware FMS subjects.
Conclusions: Contingency learning deficits represent a potentially promising and specific, but largely unstudied, psychopathological factor in FMS. Deficits in contingency learning may increase anxiety and, consequently, pain sensation. These findings have the potential to contribute to the development of novel therapeutic approaches for FMS.
© 2013 European Federation of International Association for the Study of Pain Chapters.
Conflict of interest statement
None declared.
Figures
Comment in
-
Fear-learning deficits in fibromyalgia: precursor or consequence?Eur J Pain. 2013 Oct;17(9):1265-6. doi: 10.1002/j.1532-2149.2013.00382.x. Eur J Pain. 2013. PMID: 24006368 No abstract available.
References
-
- Al Absi M, Rokke PD. Can anxiety help us tolerate pain? Pain. 1991;46:43–51. - PubMed
-
- Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, Healey LA, Kaplan SR, Liang MH, Luthra HS. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31:315–324. - PubMed
-
- Asmundson GJ, Katz J. Understanding the co-occurrence of anxiety disorders and chronic pain: State-of-the-art. Depress Anxiety. 2009;26:888–901. - PubMed
-
- Asmundson GJ, Taylor S. Role of anxiety sensitivity in pain-related fear and avoidance. J Behav Med. 1996;19:577–586. - PubMed
-
- Bartley EJ, Rhudy JL, Williams AE. Experimental assessment of affective processing in fibromyalgia. J Pain. 2009;10:1151–1160. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
