

Early antenatal care: does it make a difference to outcomes of pregnancy associated with syphilis? A systematic review and meta-analysis
- PMID: 23468875
- PMCID: PMC3585307
- DOI: 10.1371/journal.pone.0056713
Early antenatal care: does it make a difference to outcomes of pregnancy associated with syphilis? A systematic review and meta-analysis
Abstract
Objective: Despite an increase in the proportion of women who access antenatal care, mother-to-child transmission of syphilis continues to be a consequence of undiagnosed, untreated, or inadequately treated maternal syphilis. We reviewed evidence on the optimal timing of antenatal interventions to prevent mother-to-child transmission of syphilis and its associated adverse outcomes.
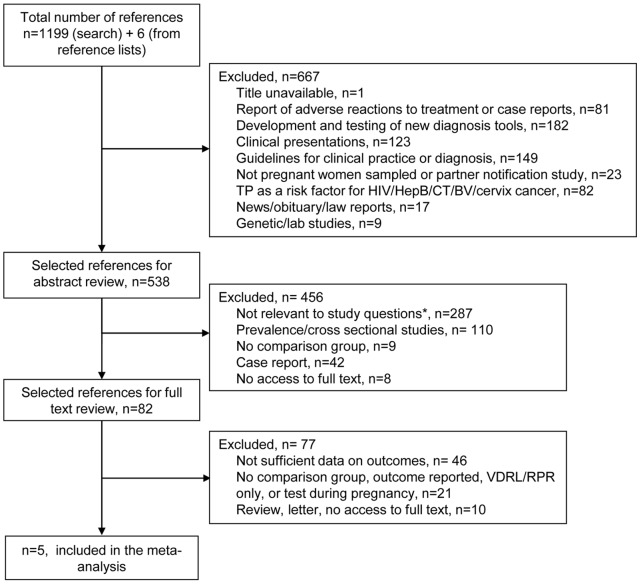
Design: Systematic review and meta-analysis of published literature. English-language articles were included if they (1) reported the gestational age at which the mother was screened or tested for syphilis; (2) reported on pregnancy outcome. No publication date limits were set.
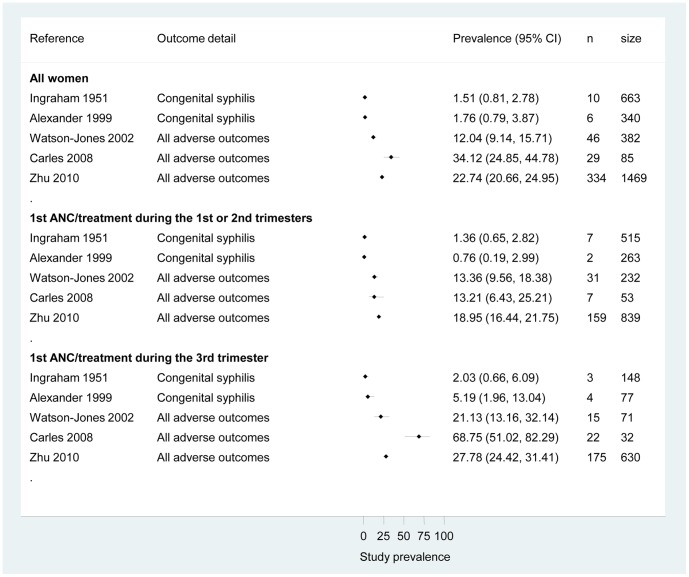
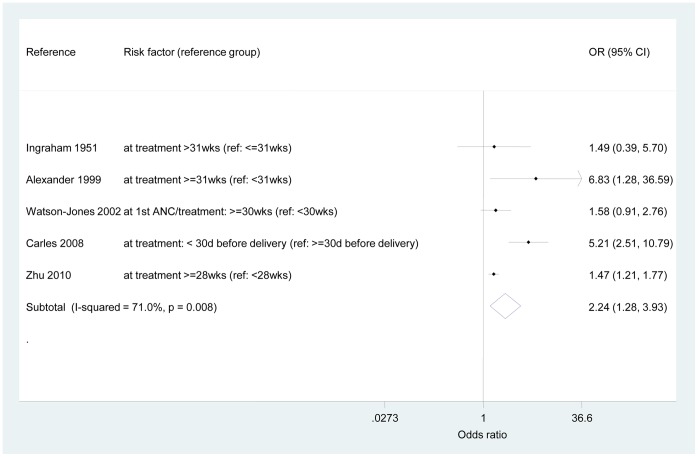
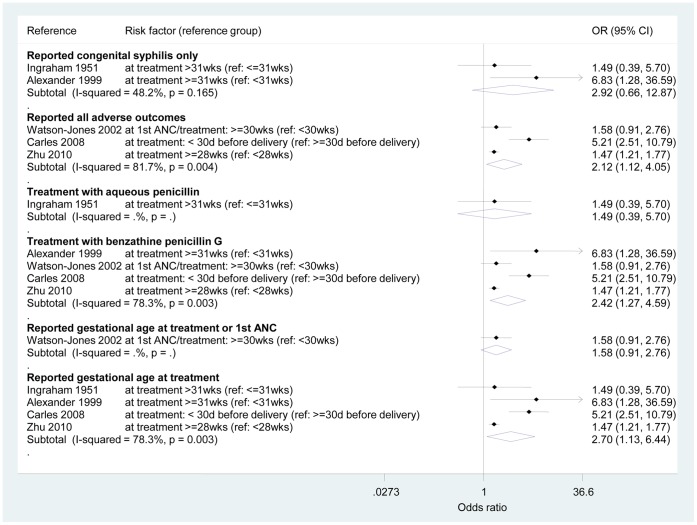
Results: We identified a total of 1,199 publications, of which 84 were selected for further review and five were included. All showed a lower prevalence of any adverse outcome among women who received an intervention (to include screening and treatment) in the first and second trimesters of pregnancy compared to the third trimester. The overall odds ratio for any adverse outcome was 2.24 (95% CI 1.28, 3.93). All sub-analyses by type of outcome presented important heterogeneity between studies, except for those studies reporting an infected infant (odds ratio 2.92, 95% CI 0.66, 12.87; I(2) = 48.2%, p = 0.165).
Conclusions: Our review has shown that the timing of antenatal care interventions makes a significant difference in the risk of having an adverse outcome due to syphilis. Women who sought care in the first two trimesters of their pregnancy, and received the appropriate intervention, were more likely to have a healthy infant, compared to women screened and treated in the third trimester. Encouraging ALL pregnant women to seek care in the first two trimesters of their pregnancy should be a priority for health programmes. For interventions to be effective within these health programmes, health systems and community engagement programmes need to be strengthened to enable pregnant women to seek antenatal care early.
Conflict of interest statement
Figures
References
-
- CDC (1989) Congenital syphilis. New York City, 1986–1988. MMWR 38: 825–829. - PubMed
-
- Gust DA, Levine WC, St Louis ME, Braxton J, Berman SM (2002) Mortality associated with congenital syphilis in the United States, 1992–1998. Pediatrics 109: E79–79. - PubMed
-
- Liu JB, Hong FC, Pan P, Zhou H, Yang F, et al. (2010) A risk model for congenital syphilis in infants born to mothers with syphilis treated in gestation: a prospective cohort study. Sex Transm Infect 86: 292–296. - PubMed
-
- Schmid GP, Stoner BP, Hawkes S, Broutet N (2007) The need and plan for global elimination of congenital syphilis. Sex Transm Dis 34: S5–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
