

How effective is school-based deworming for the community-wide control of soil-transmitted helminths?
- PMID: 23469293
- PMCID: PMC3585037
- DOI: 10.1371/journal.pntd.0002027
How effective is school-based deworming for the community-wide control of soil-transmitted helminths?
Abstract
Background: The London Declaration on neglected tropical diseases was based in part on a new World Health Organization roadmap to "sustain, expand and extend drug access programmes to ensure the necessary supply of drugs and other interventions to help control by 2020". Large drug donations from the pharmaceutical industry form the backbone to this aim, especially for soil-transmitted helminths (STHs) raising the question of how best to use these resources. Deworming for STHs is often targeted at school children because they are at greatest risk of morbidity and because it is remarkably cost-effective. However, the impact of school-based deworming on transmission in the wider community remains unclear.
Methods: We first estimate the proportion of parasites targeted by school-based deworming using demography, school enrolment, and data from a small number of example settings where age-specific intensity of infection (either worms or eggs) has been measured for all ages. We also use transmission models to investigate the potential impact of this coverage on transmission for different mixing scenarios.
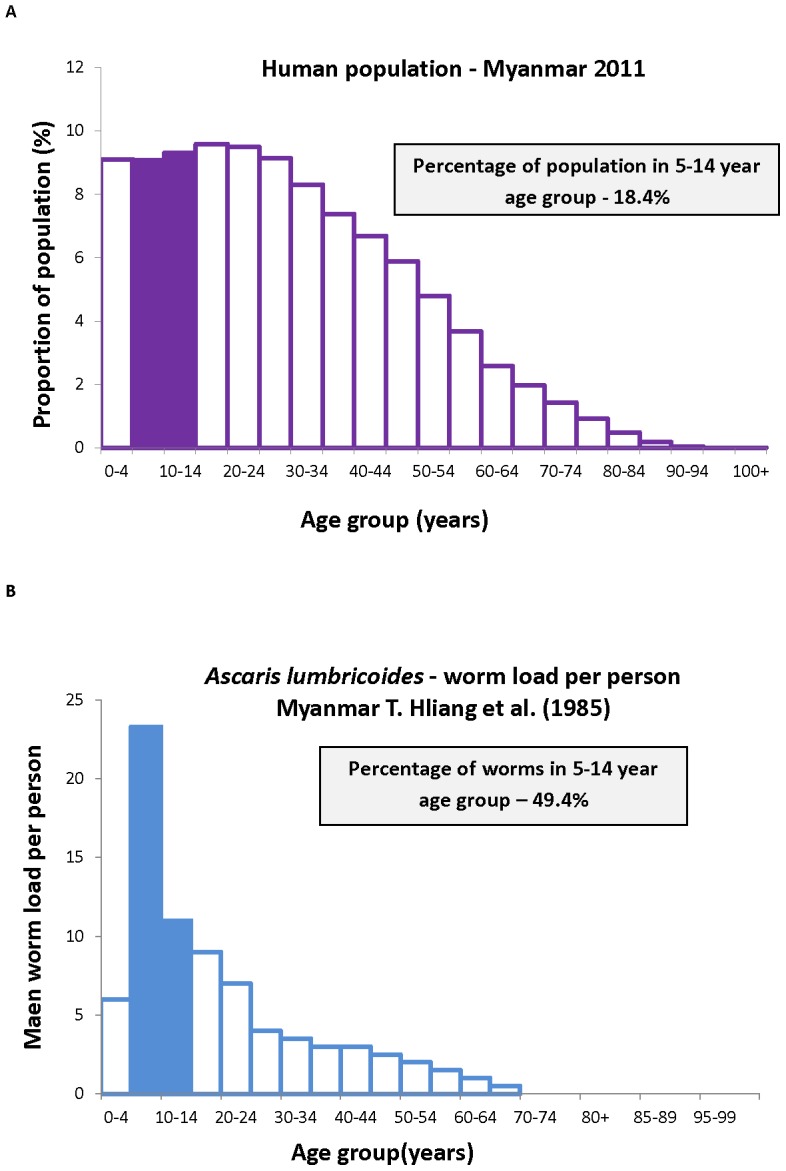
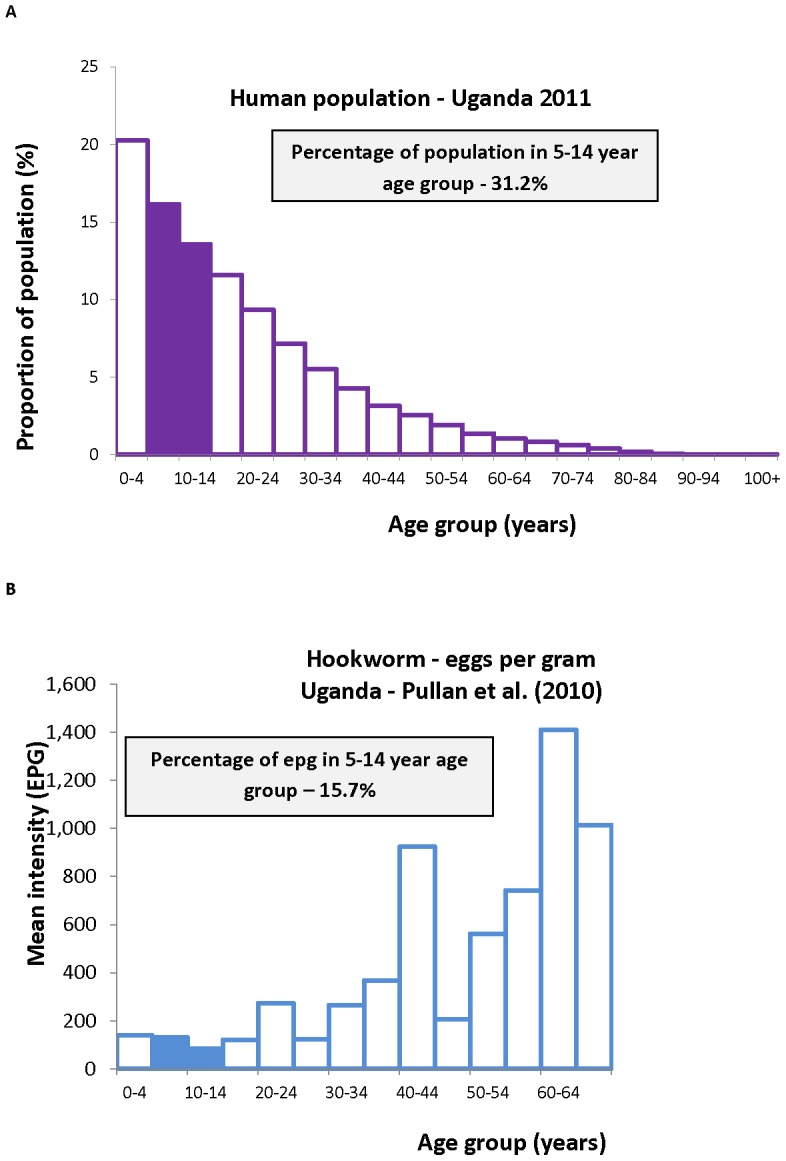
Principal findings: In the example settings <30% of the population are 5 to <15 years old. Combining this demography with the infection age-intensity profile we estimate that in one setting school children output as little as 15% of hookworm eggs, whereas in another setting they harbour up to 50% of Ascaris lumbricoides worms (the highest proportion of parasites for our examples). In addition, it is estimated that from 40-70% of these children are enrolled at school.
Conclusions: These estimates suggest that, whilst school-based programmes have many important benefits, the proportion of infective stages targeted by school-based deworming may be limited, particularly where hookworm predominates. We discuss the consequences for transmission for a range of scenarios, including when infective stages deposited by children are more likely to contribute to transmission than those from adults.
Conflict of interest statement
Roy M. Anderson is non-executive member of the board of GlaxoSmithKline (GSK). GlaxoSmithKline provided no financial support for the work and played no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Figures
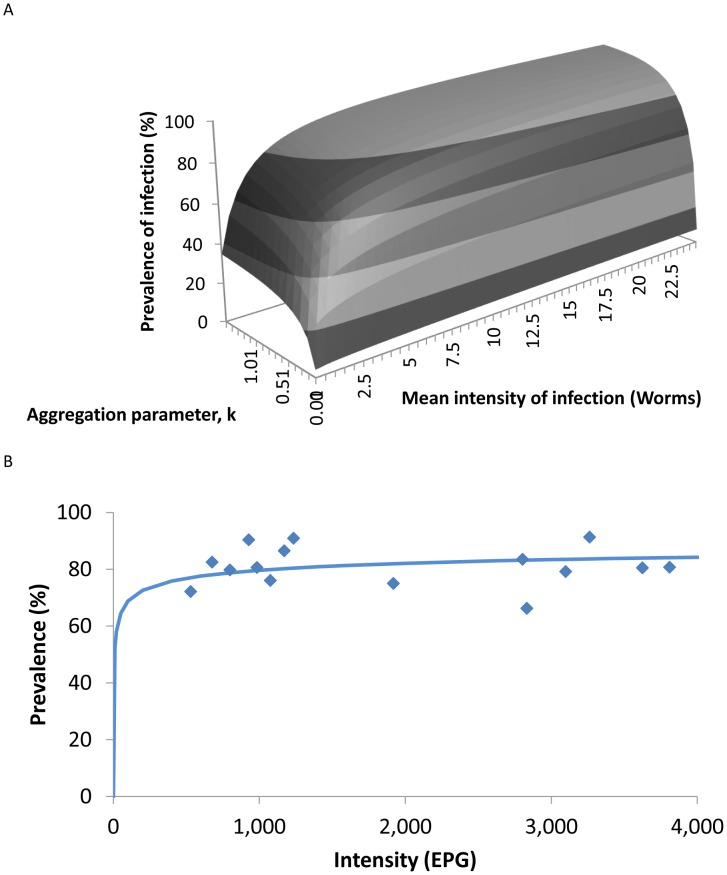
 , the prevalence of infection,
, the prevalence of infection,  , and the negative binomial aggregation parameter,
, and the negative binomial aggregation parameter,  as described by the relationship in equation 1. B Relationship between the prevalence and intensity of infection as observed in a study of A. lumbricoides
. The solid line is the predicted relationship between mean prevalence of infection and worm burden described in equation 1 and plotted in A fitted to estimate the aggregation parameter,
as described by the relationship in equation 1. B Relationship between the prevalence and intensity of infection as observed in a study of A. lumbricoides
. The solid line is the predicted relationship between mean prevalence of infection and worm burden described in equation 1 and plotted in A fitted to estimate the aggregation parameter,  = 0.194.
= 0.194.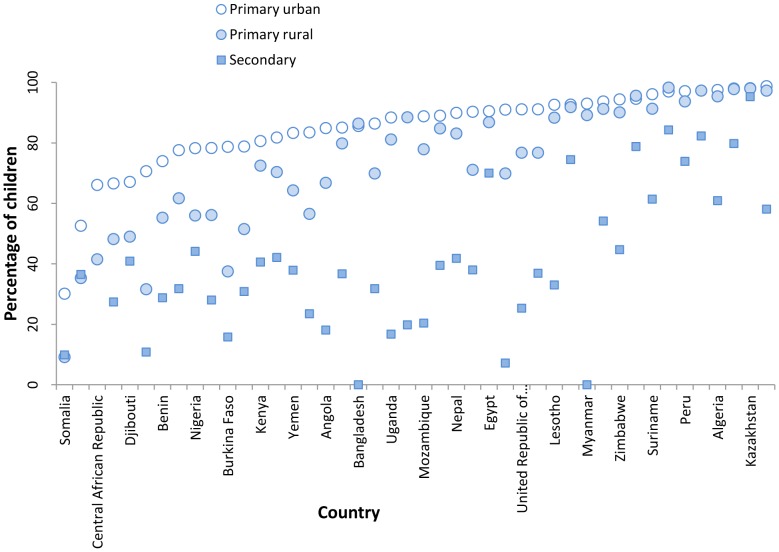
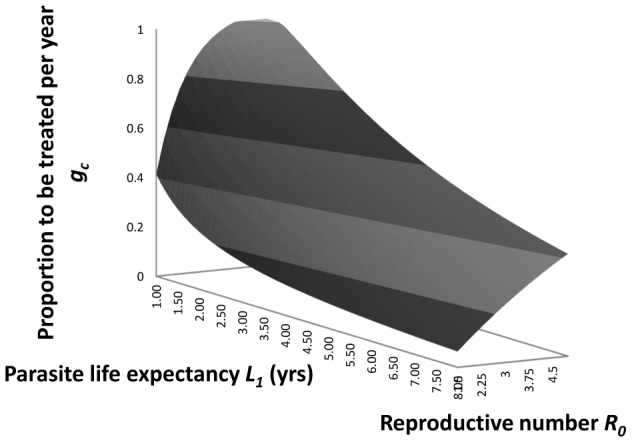
 , per annum with efficacy,
, per annum with efficacy,  , 0.9, and the basic reproductive number,
, 0.9, and the basic reproductive number,  , and parasite life expectancy,
, and parasite life expectancy,  in years (from equation 11 in the main text).
in years (from equation 11 in the main text).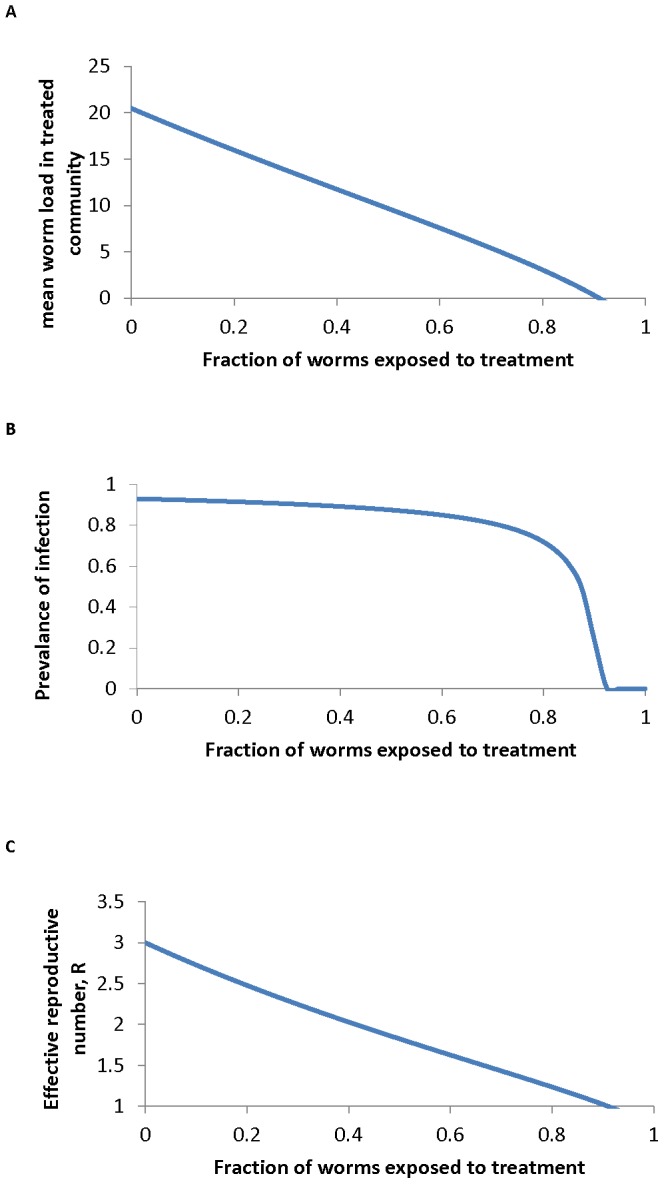
 , on A the mean worm burden
, on A the mean worm burden  , B the prevalence of infection,
, B the prevalence of infection,  and C the effective reproductive number
and C the effective reproductive number  , as described in equation 10. Parameter values are set for A. lumbricoides as follows:
, as described in equation 10. Parameter values are set for A. lumbricoides as follows:  = 0.81,
= 0.81,  = 3,
= 3,  = 1 yr,
= 1 yr,  = 0.967 and
= 0.967 and  = 0.95.
= 0.95.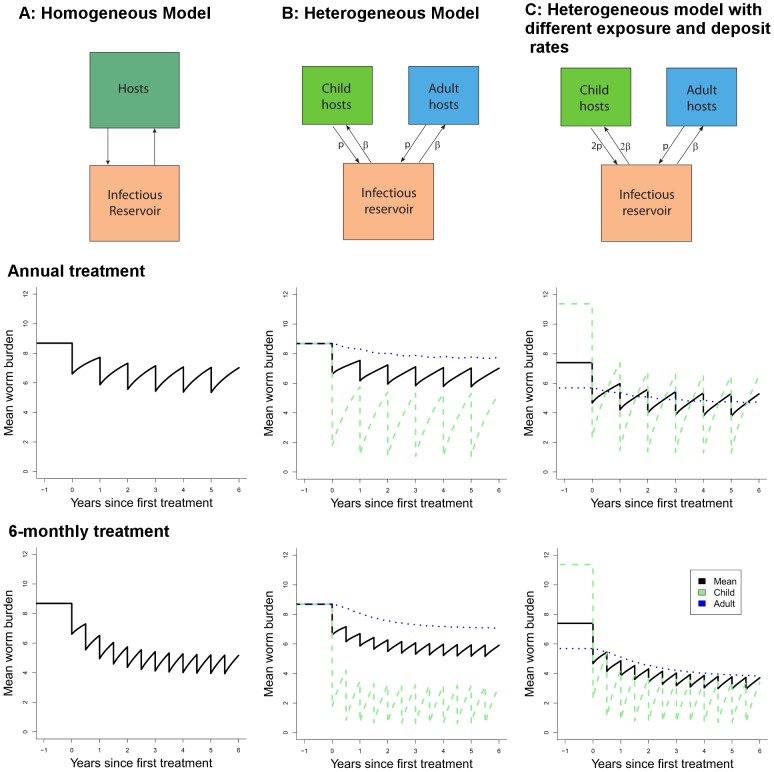
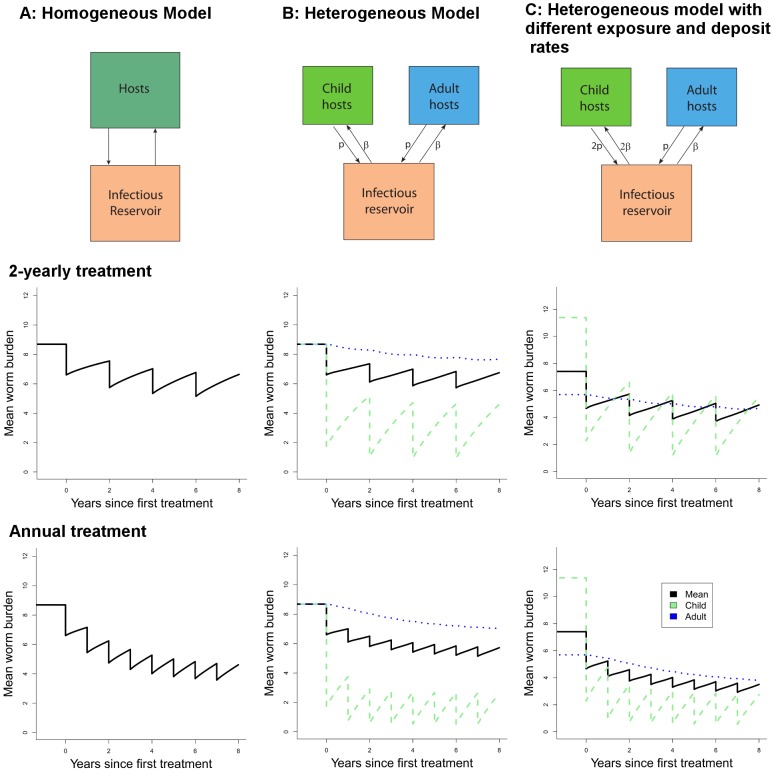
 = 3, and worm lifespan is 2.5 years. Other parameters as in Figure 7. The two rows represent two-yearly and yearly treatment respectively.
= 3, and worm lifespan is 2.5 years. Other parameters as in Figure 7. The two rows represent two-yearly and yearly treatment respectively.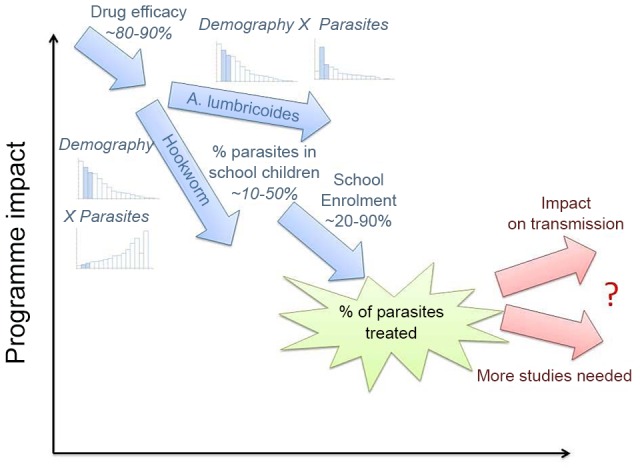
References
-
- WHO (2012) Accelerating work to overcome the global impact of neglected tropical diseases - A roadmap for implementation. Geneva: World Health Organization.
-
- WHO (2011) Soil-transmitted helminthiases: estimates of the number of children needing preventive chemotherapy and number treated, 2009. Wkly Epidemiol Rec 86: 257–266. - PubMed
-
- WHO (2006) Preventive Chemotheraphy in Human Helminthiasis. Geneva, Switzerland: World Health Organization.
-
- Keiser J, Utzinger J (2008) Efficacy of current drugs against soil-transmitted helminth infections: systematic review and meta-analysis. JAMA 299: 1937–1948. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
