

Risk factors associated with mortality after Roux-en-Y gastric bypass surgery
- PMID: 23470583
- PMCID: PMC4075503
- DOI: 10.1097/SLA.0b013e31828a0ee4
Risk factors associated with mortality after Roux-en-Y gastric bypass surgery
Abstract
Objective: We sought to identify the major risk factors associated with mortality in Roux-en-Y gastric bypass (RYGB) surgery.
Background: Bariatric surgery has become an established treatment for extreme obesity. Bariatric surgery mortality has steadily declined with current rates of less than 0.5%. However, significant variation in the mortality rates has been reported for specific patient cohorts and among bariatric centers.
Methods: Clinical outcome data from 185,315 bariatric surgery patients from the Bariatric Outcome Longitudinal Database were reviewed. Of these, 157,559 patients had either documented 30 or more day follow-up data, including mortality. Multiple demographic, socioeconomic, and clinical factors were analyzed by univariate analysis for their association with 30-day mortality after gastric bypass. Variables found to be significant were entered into a multiple logistic regression model to identify factors independently associated with 30-day mortality. On the basis of these results, a RYGB mortality risk score was developed.
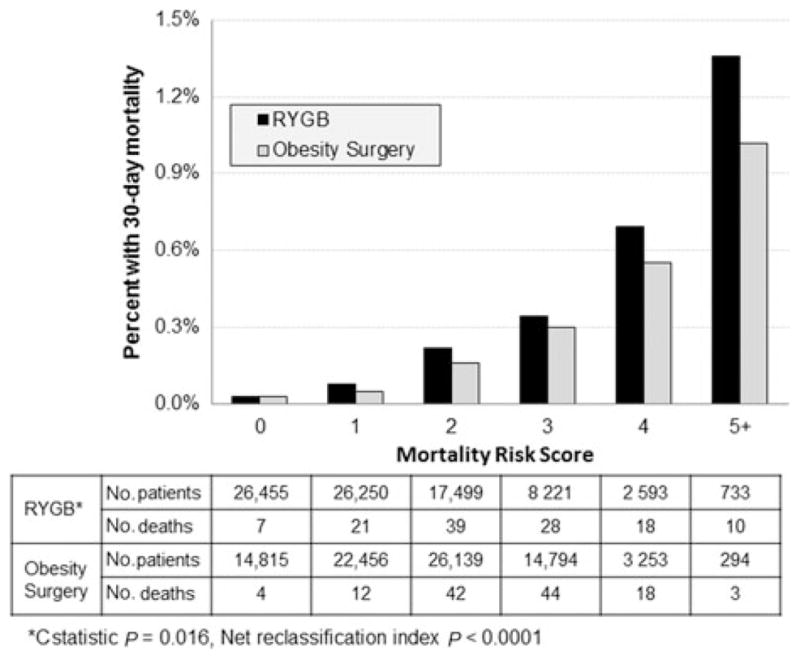
Results: The overall 30-day mortality rate for the entire bariatric surgery cohort was 0.1%. Of the 81,751 RYGB patients, the mortality rate was 0.15%. Factors significantly associated with 30-day gastric bypass mortality included increasing body mass index (BMI) (P<0.0001), increasing age (P<0.005), male gender (P<0.001), pulmonary hypertension (P<0.0001), congestive heart failure (P=0.0008), and liver disease (P=0.038). When the RYGB risk score was applied, a significant trend (P<0.0001) between increasing risk score and mortality rate is found.
Conclusions: Increasing BMI, increasing age, male gender, pulmonary hypertension, congestive heart failure, and liver disease are risk factors for 30-day mortality after RYGB. The RYGB risk score can be used to determine patients at greater risk for mortality after RYGB surgery.
Figures
References
-
- NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med. 1991;115:956–961. - PubMed
-
- Finks JF, Kole KL, Yenumula PR, et al. Predicting risk for serious complications with bariatric surgery: results from the Michigan Bariatric Surgery Collaborative. Ann Surg. 2011;254:633–640. - PubMed
-
- Gupta PK, Franck C, Miller WJ, et al. Development and validation of a bariatric surgery morbidity risk calculator using the prospective, multicenter NSQIP dataset. J Am Coll Surg. 2011;212:301–309. - PubMed
-
- Nguyen NT, Masoomi H, Laugenour K, et al. Predictive factors of mortality in bariatric surgery: data from the Nationwide Inpatient Sample. Surgery. 2011;150:347–351. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
