

Stents are associated with increased risk of respiratory infections in patients undergoing airway interventions for malignant airways disease
- PMID: 23471176
- PMCID: PMC4694097
- DOI: 10.1378/chest.12-1721
Stents are associated with increased risk of respiratory infections in patients undergoing airway interventions for malignant airways disease
Abstract
Background: Long-term complications of therapeutic bronchoscopy include infections and airway restenosis due to tumor. No studies have compared the incidence rates of infection in patients with stents with those without stents. We hypothesized that patients with stents would have a higher incidence of lower respiratory tract infections than would patients without stents.
Methods: We conducted a retrospective cohort study, covering the period September 2009 to August 2011, of patients who had therapeutic bronchoscopy for malignant airways disease. Outcomes recorded were lower respiratory tract infection and airway restenosis by tumor.
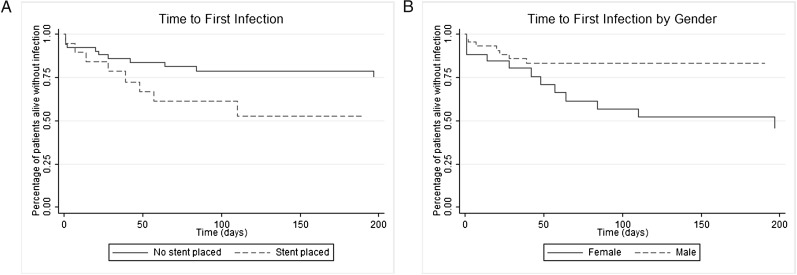
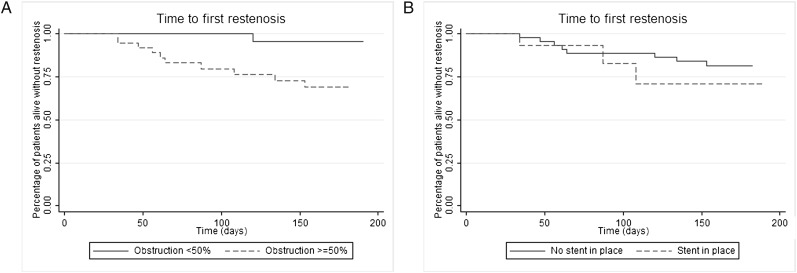
Results: Seventy-two patients had therapeutic bronchoscopy for malignant airways disease. Twenty-four of these patients had one or more stents placed. Twenty-three of the 72 patients (32%) developed lower respiratory tract infections. Stents were associated with an increased risk of infection (hazard ratio [HR], 3.76; 95% CI, 1.57-8.99; P = .003). The incidence rate of lower respiratory tract infection was 0.0057 infections per person-day in patients with stents vs 0.0011 infections per person-day in patients without stents. The incidence rate difference, 0.0046 infections per person-day, was significant (95% CI, 0.0012-0.0081; P = .0002). Restenosis due to tumor overgrowth was associated with more severe obstruction at baseline (obstruction ≥ 50% vs < 50% preprocedure; HR, 13.71; 95% CI, 1.75-107.55; P = .013).
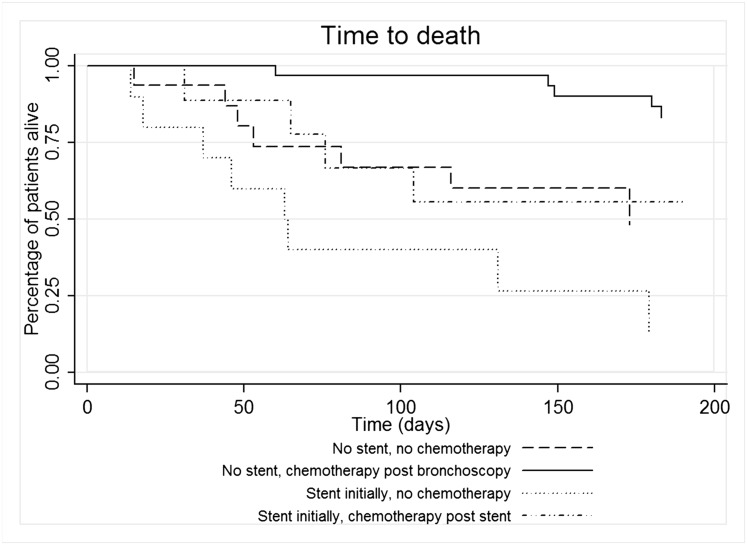
Conclusion: Therapeutic bronchoscopy with stent placement is associated with a higher risk of infection than is therapeutic bronchoscopy alone. If ablative techniques reopen the airway and there is a good chance that the tumor may respond to chemotherapy and/or radiation, a strategy of initially holding off on stenting may be warranted.
Figures
References
-
- Stöhr S, Bolliger CT. Stents in the management of malignant airway obstruction. Monaldi Arch Chest Dis. 1999;54(3):264-268. - PubMed
-
- Alazemi S, Lunn W, Majid A, et al. Outcomes, health-care resources use, and costs of endoscopic removal of metallic airway stents. Chest. 2010;138(2):350-356. - PubMed
-
- Agrafiotis M, Siempos II, Falagas ME. Infections related to airway stenting: a systematic review. Respiration. 2009;78(1):69-74. - PubMed
-
- Breitenbücher A, Chhajed PN, Brutsche MH, Mordasini C, Schilter D, Tamm M. Long-term follow-up and survival after Ultraflex stent insertion in the management of complex malignant airway stenoses. Respiration. 2008;75(4):443-449. - PubMed
-
- Wassermann K. How much incidence is enough? Chest. 2001;120(2):686-687. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
