

Sagging eye syndrome: connective tissue involution as a cause of horizontal and vertical strabismus in older patients
- PMID: 23471194
- PMCID: PMC3999699
- DOI: 10.1001/jamaophthalmol.2013.783
Sagging eye syndrome: connective tissue involution as a cause of horizontal and vertical strabismus in older patients
Abstract
Importance: Recognition of sagging eye syndrome (SES) as the cause of chronic or acute acquired diplopia may avert neurologic evaluation and imaging in most cases.
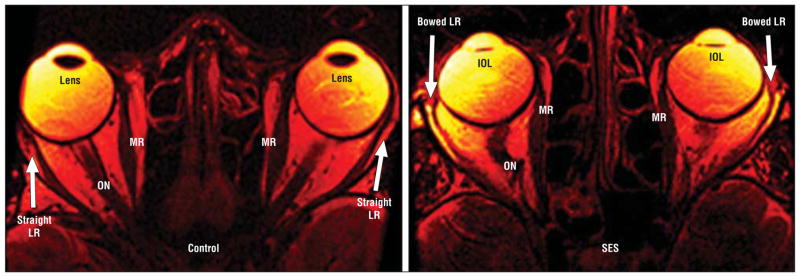
Objectives: To determine whether SES results from inferior shift of lateral rectus (LR) extraocular muscle (EOM) pulleys and to investigate anatomic correlates of strabismus in SES.
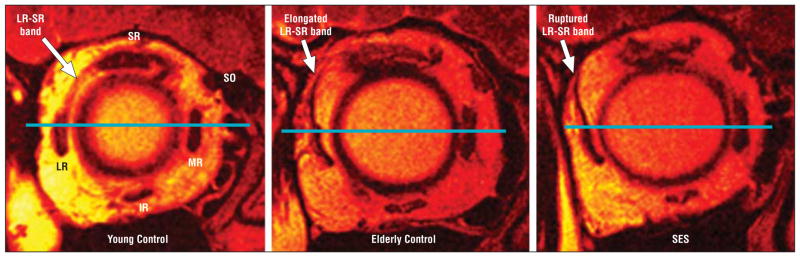
Design and setting: We used magnetic resonance imaging to evaluate rectus EOMs, pulleys, and the LR-superior rectus (SR) band ligament at an eye institute.
Participants: Patients with acquired diplopia suspected of having SES. We studied 56 orbits of 11 men and 17 women (mean [SD] age of 69.4 [11.9] years) clinically diagnosed with SES. Data were obtained from 25 orbits of 14 control participants age-matched to SES and from 52 orbits of 28 younger controls (23 [4.6] years).
Main outcome measures: Rectus pulley locations compared with age-matched norms and lengths of the LR-SR band ligament and rectus EOMs. Data were correlated with facial features, binocular alignment, and fundus torsion.
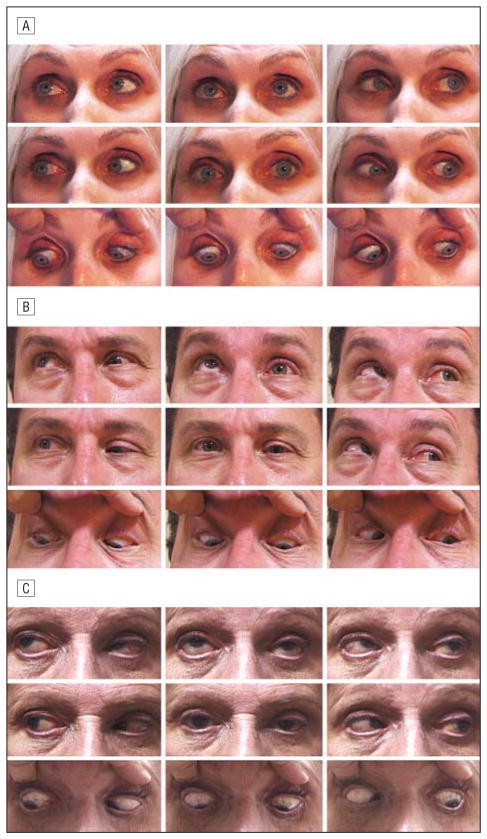
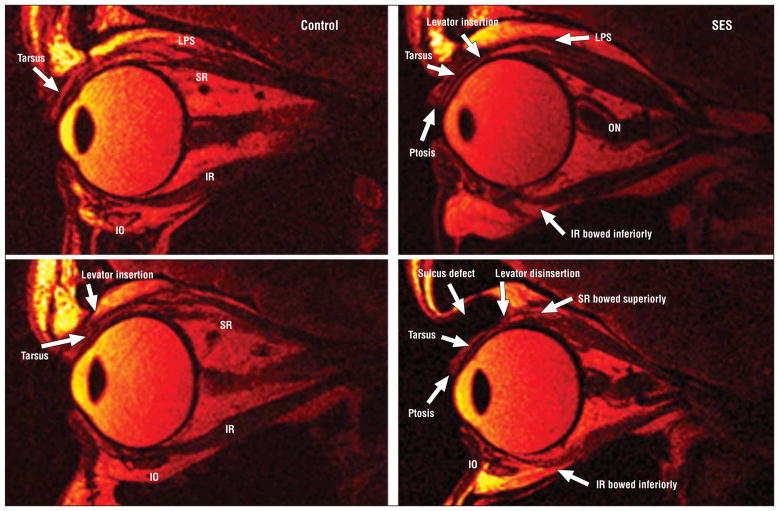
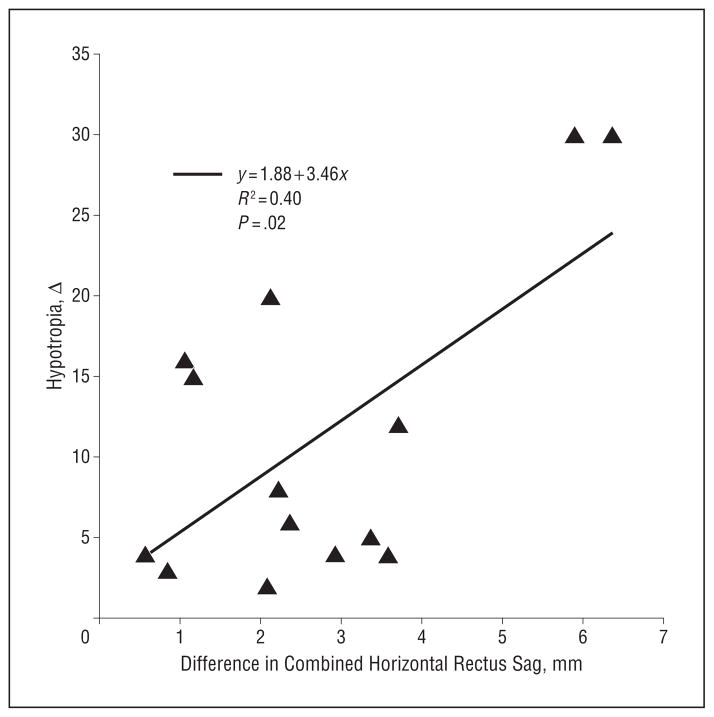
Results: Patients with SES commonly exhibited blepharoptosis and superior sulcus defect. Significant inferolateral LR pulley displacement was confirmed in SES, but the spectrum of abnormalities was extended to peripheral displacement of all other rectus pulleys and lateral displacement of the inferior rectus pulley, with elongation of rectus EOMs (P < .001). Symmetrical LR sag was associated with divergence paralysis esotropia and asymmetrical LR sag greater than 1 mm with cyclovertical strabismus. The LR-SR band was ruptured in 91% of patients with SES.
Conclusions and relevance: Widespread rectus pulley displacement and EOM elongation, associated with LR-SR band rupture, causes acquired vertical and horizontal strabismus. Small-angle esotropia or hypertropia may result from common involutional changes in EOMs and orbital connective tissues that may be suspected from features evident on external examination.
Conflict of interest statement
Figures
References
-
- Demer JL. More respect for connective tissues. J AAPOS. 2008;12(1):5–6. - PubMed
-
- Kono R, Poukens V, Demer JL. Quantitative analysis of the structure of the human extraocular muscle pulley system. Invest Ophthalmol Vis Sci. 2002;43 (9):2923–2932. - PubMed
-
- Frueh BR. The mechanistic classification of ptosis. Ophthalmology. 1980;87(10):1019–1021. - PubMed
-
- Clark RA, Isenberg SJ. The range of ocular movements decreases with aging. J AAPOS. 2001;5(1):26–30. - PubMed
-
- Clark RA, Demer JL. Effect of aging on human rectus extraocular muscle paths demonstrated by magnetic resonance imaging. Am J Ophthalmol. 2002;134 (6):872–878. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
