

Management of anemia in children receiving chronic peritoneal dialysis
- PMID: 23471197
- PMCID: PMC3609132
- DOI: 10.1681/ASN.2012050433
Management of anemia in children receiving chronic peritoneal dialysis
Abstract
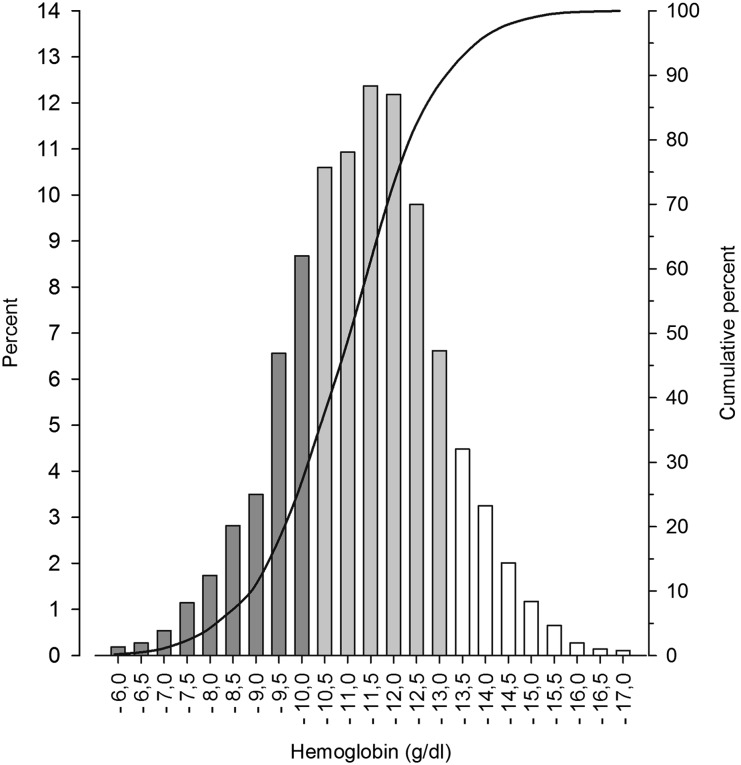
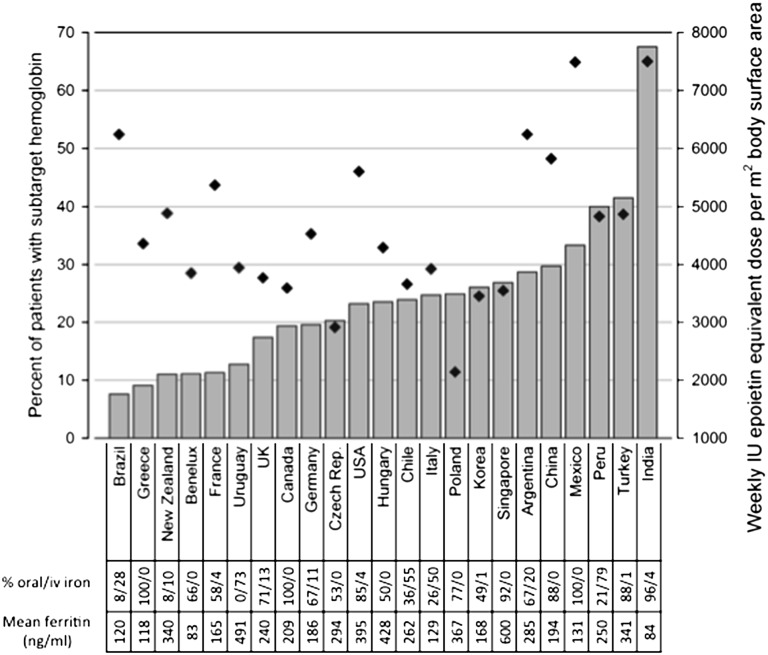
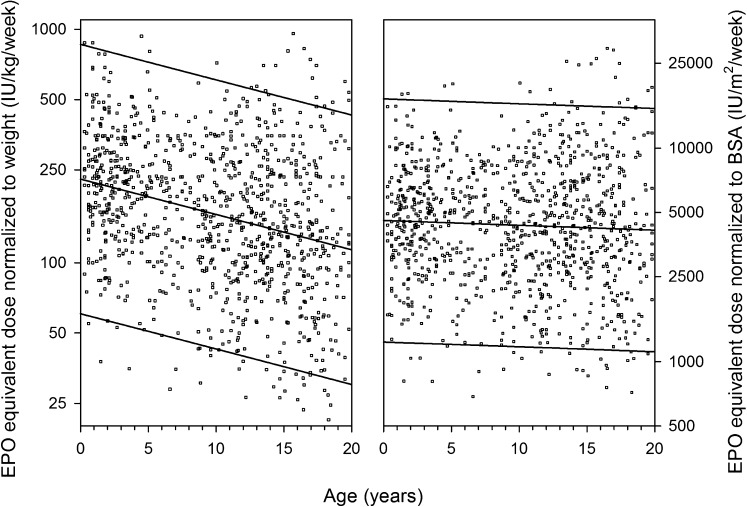
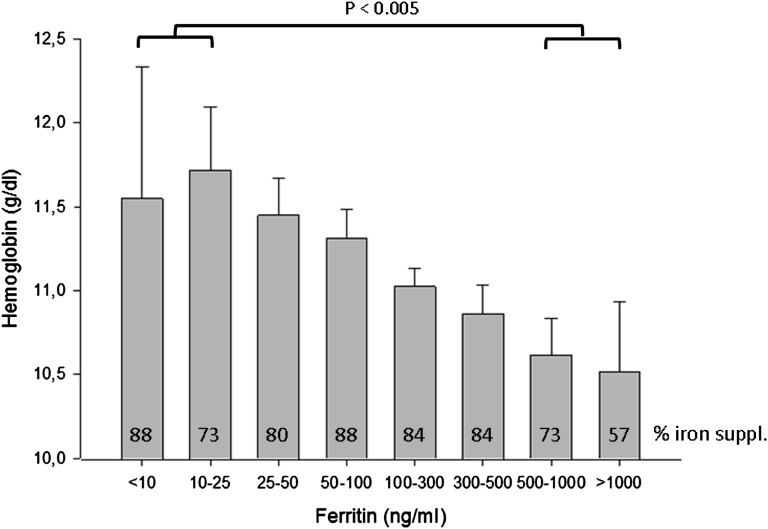
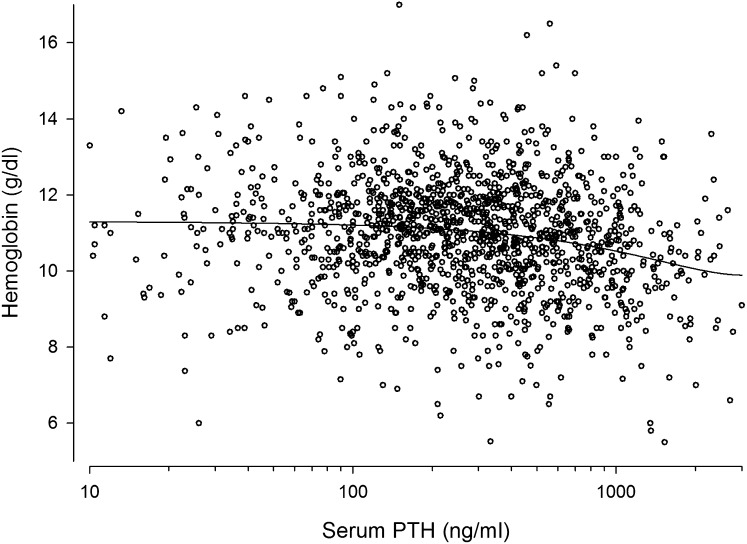
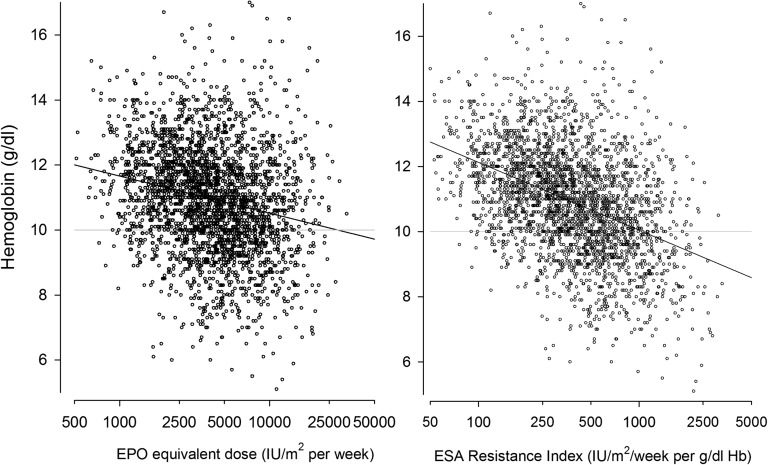
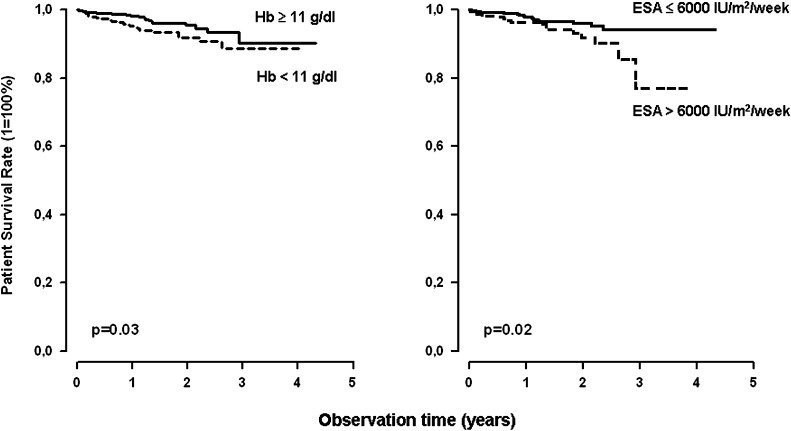
Little information exists regarding the efficacy, modifiers, and outcomes of anemia management in children with CKD or ESRD. We assessed practices, effectors, and outcomes of anemia management in 1394 pediatric patients undergoing peritoneal dialysis (PD) who were prospectively followed in 30 countries. We noted that 25% of patients had hemoglobin levels below target (<10 g/dl or <9.5 g/dl in children older or younger than 2 years, respectively), with significant regional variation; levels were highest in North America and Europe and lowest in Asia and Turkey. Low hemoglobin levels were associated with low urine output, low serum albumin, high parathyroid hormone, high ferritin, and the use of bioincompatible PD fluid. Erythropoiesis-stimulating agents (ESAs) were prescribed to 92% of patients, and neither the type of ESA nor the dosing interval appeared to affect efficacy. The weekly ESA dose inversely correlated with age when scaled to weight but did not correlate with age when normalized to body surface area. ESA sensitivity was positively associated with residual diuresis and serum albumin and inversely associated with serum parathyroid hormone and ferritin. The prevalence of hypertension and left ventricular hypertrophy increased with the degree of anemia. Patient survival was positively associated with achieved hemoglobin and serum albumin and was inversely associated with ESA dose. In conclusion, control of anemia in children receiving long-term PD varies by region. ESA requirements are independent of age when dose is scaled to body surface area, and ESA resistance is associated with inflammation, fluid retention, and hyperparathyroidism. Anemia and high ESA dose requirements independently predict mortality.
Figures
References
-
- McMahon LP, Mason K, Skinner SL, Burge CM, Grigg LE, Becker GJ: Effects of haemoglobin normalization on quality of life and cardiovascular parameters in end-stage renal failure. Nephrol Dial Transplant 15: 1425–1430, 2000 - PubMed
-
- Fink J, Blahut S, Reddy M, Light P: Use of erythropoietin before the initiation of dialysis and its impact on mortality. Am J Kidney Dis 37: 348–355, 2001 - PubMed
-
- Warady BA, Ho M: Morbidity and mortality in children with anemia at initiation of dialysis. Pediatr Nephrol 18: 1055–1062, 2003 - PubMed
-
- Besarab A, Bolton WK, Browne JK, Egrie JC, Nissenson AR, Okamoto DM, Schwab SJ, Goodkin DA: The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med 339: 584–590, 1998 - PubMed
-
- Singh AK, Szczech L, Tang KL, Barnhart H, Sapp S, Wolfson M, Reddan D, CHOIR Investigators : Correction of anemia with epoetin alfa in chronic kidney disease. N Engl J Med 355: 2085–2098, 2006 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
