

Natriuretic peptide-guided therapy in chronic heart failure: a meta-analysis of 2,686 patients in 12 randomized trials
- PMID: 23472172
- PMCID: PMC3589263
- DOI: 10.1371/journal.pone.0058287
Natriuretic peptide-guided therapy in chronic heart failure: a meta-analysis of 2,686 patients in 12 randomized trials
Erratum in
- PLoS One. 2014;9(4):e96706
Abstract
Background: The role of cardiac natriuretic peptides in the management of patients with chronic heart failure (HF) remains uncertain. The purpose of this study was to evaluate whether natriuretic peptide-guided therapy, compared to clinically-guided therapy, improves mortality and hospitalization rate in patients with chronic HF.
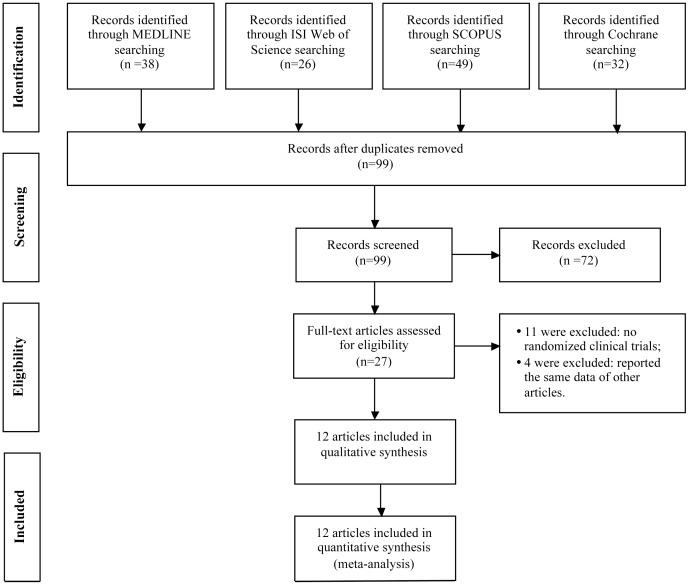
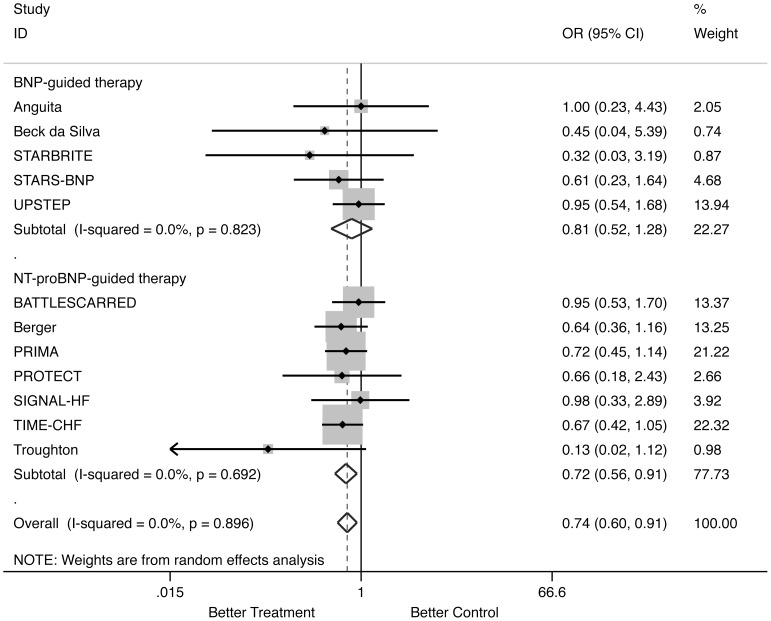
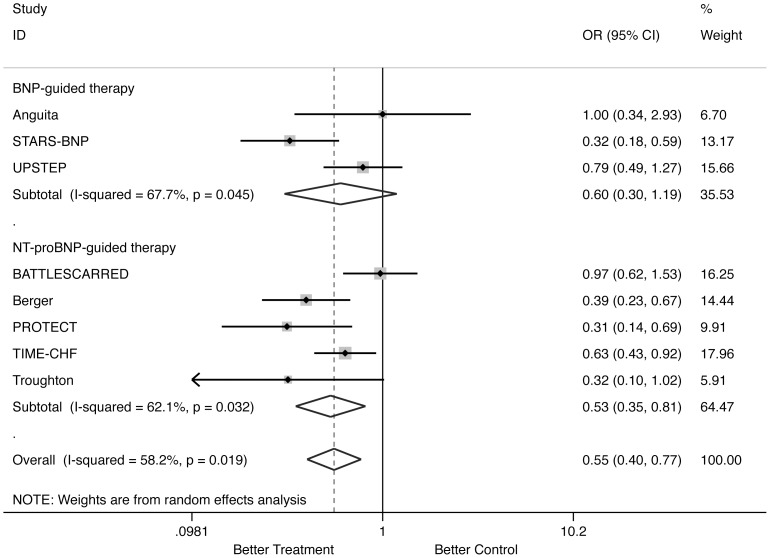
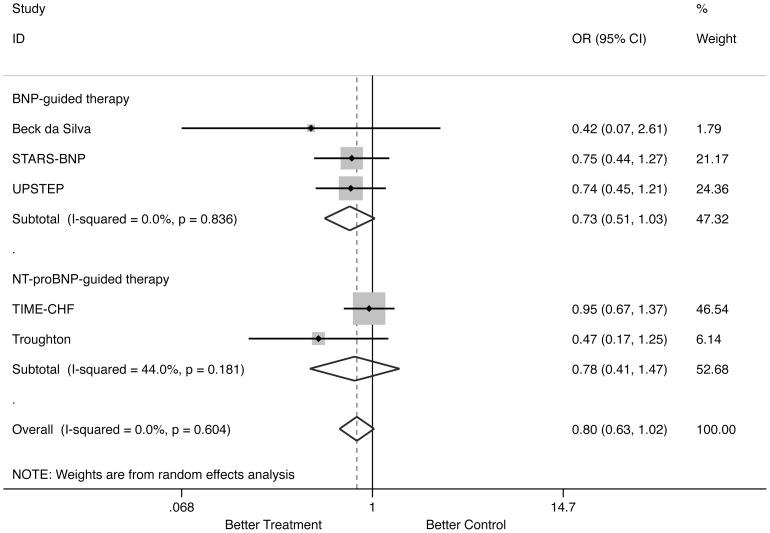
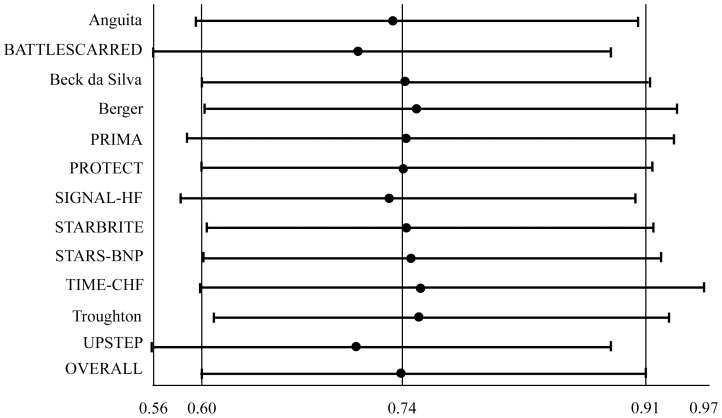
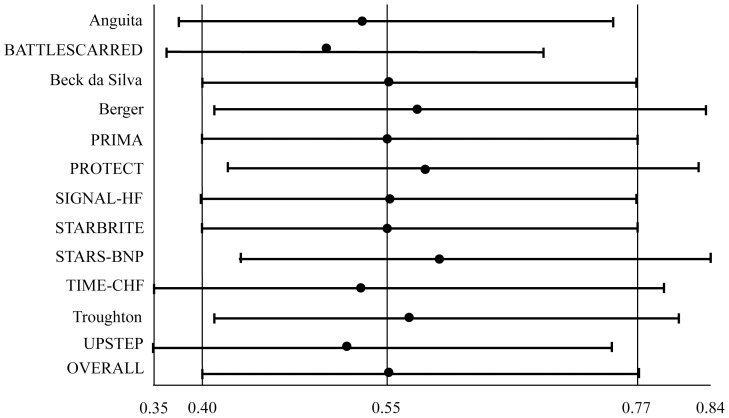
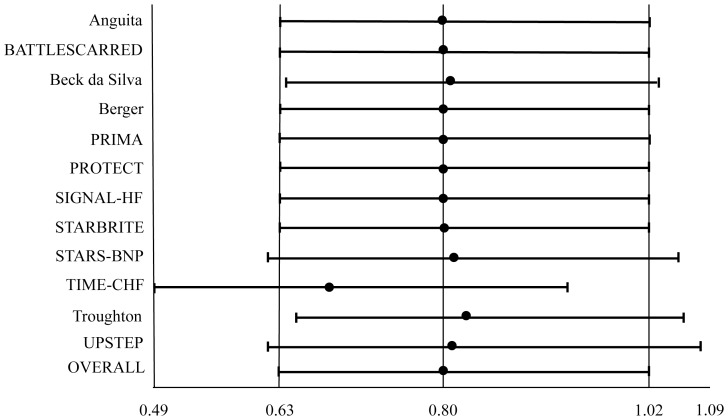
Methodology/principal findings: MEDLINE, Cochrane, ISI Web of Science and SCOPUS databases were searched for articles reporting natriuretic peptide-guided therapy in HF until August 2012. All randomized trials reporting clinical end-points (all-cause mortality and/or HF-related hospitalization and/or all-cause hospitalization) were included. Meta-analysis was performed to assess the influence of treatment on outcomes. Sensitivity analysis was performed to test the influence of potential effect modifiers and of each trial included in meta-analysis on results. Twelve trials enrolling 2,686 participants were included. Natriuretic peptide-guided therapy (either B-type natriuretic peptide [BNP]- or N-terminal pro-B-type natriuretic peptide [NT-proBNP]-guided therapy) significantly reduced all-cause mortality (Odds Ratio [OR]:0.738; 95% Confidence Interval [CI]:0.596 to 0.913; p = 0.005) and HF-related hospitalization (OR:0.554; CI:0.399 to 0.769; p = 0.000), but not all-cause hospitalization (OR:0.803; CI:0.629 to 1.024; p = 0.077). When separately assessed, NT-proBNP-guided therapy significantly reduced all-cause mortality (OR:0.717; CI:0.563 to 0.914; p = 0.007) and HF-related hospitalization (OR:0.531; CI:0.347 to 0.811; p = 0.003), but not all-cause hospitalization (OR:0.779; CI:0.414 to 1.465; p = 0.438), whereas BNP-guided therapy did not significantly reduce all-cause mortality (OR:0.814; CI:0.518 to 1.279; p = 0.371), HF-related hospitalization (OR:0.599; CI:0.303 to 1.187; p = 0.142) or all-cause hospitalization (OR:0.726; CI:0.509 to 1.035; p = 0.077). [corrected].
Conclusions/significance: Use of cardiac peptides to guide pharmacologic therapy significantly reduces mortality and HF related hospitalization in patients with chronic HF. In particular, NT-proBNP-guided therapy reduced all-cause mortality and HF-related hospitalization but not all-cause hospitalization, whereas BNP-guided therapy did not significantly reduce both mortality and morbidity.
Conflict of interest statement
Figures
Similar articles
-
Changes of natriuretic peptides predict hospital admissions in patients with chronic heart failure: a meta-analysis.JACC Heart Fail. 2014 Apr;2(2):148-58. doi: 10.1016/j.jchf.2013.11.007. JACC Heart Fail. 2014. PMID: 24720923 Review.
-
Effect of Natriuretic Peptide-Guided Therapy on Hospitalization or Cardiovascular Mortality in High-Risk Patients With Heart Failure and Reduced Ejection Fraction: A Randomized Clinical Trial.JAMA. 2017 Aug 22;318(8):713-720. doi: 10.1001/jama.2017.10565. JAMA. 2017. PMID: 28829876 Free PMC article. Clinical Trial.
-
NT-proBNP (N-Terminal pro-B-Type Natriuretic Peptide)-Guided Therapy in Acute Decompensated Heart Failure: PRIMA II Randomized Controlled Trial (Can NT-ProBNP-Guided Therapy During Hospital Admission for Acute Decompensated Heart Failure Reduce Mortality and Readmissions?).Circulation. 2018 Apr 17;137(16):1671-1683. doi: 10.1161/CIRCULATIONAHA.117.029882. Epub 2017 Dec 14. Circulation. 2018. PMID: 29242350 Clinical Trial.
-
N-Terminal Pro-B-Type Natriuretic Peptide-Guided Therapy in Chronic Heart Failure Reduces Repeated Hospitalizations-Results From TIME-CHF.J Card Fail. 2017 May;23(5):382-389. doi: 10.1016/j.cardfail.2017.02.001. Epub 2017 Feb 13. J Card Fail. 2017. PMID: 28232046 Clinical Trial.
-
B-type natriuretic peptide-guided chronic heart failure therapy: a meta-analysis of 11 randomised controlled trials.Heart Lung Circ. 2013 Oct;22(10):852-60. doi: 10.1016/j.hlc.2013.03.077. Epub 2013 Apr 17. Heart Lung Circ. 2013. PMID: 23602555 Review.
Cited by
-
Novel Biomarkers in Heart Failure Beyond Natriuretic Peptides - The Case for Soluble ST2.Eur Cardiol. 2015 Jul;10(1):37-41. doi: 10.15420/ecr.2015.10.01.37. Eur Cardiol. 2015. PMID: 30310421 Free PMC article. Review.
-
Left ventricular systolic function and the pattern of late-gadolinium-enhancement independently and additively predict adverse cardiac events in muscular dystrophy patients.J Cardiovasc Magn Reson. 2014 Sep 25;16(1):81. doi: 10.1186/s12968-014-0081-1. J Cardiovasc Magn Reson. 2014. PMID: 25315351 Free PMC article.
-
Hypothyroidism and its rapid correction alter cardiac remodeling.PLoS One. 2014 Oct 15;9(10):e109753. doi: 10.1371/journal.pone.0109753. eCollection 2014. PLoS One. 2014. PMID: 25333636 Free PMC article.
-
Rationale and design of the GUIDE-IT study: Guiding Evidence Based Therapy Using Biomarker Intensified Treatment in Heart Failure.JACC Heart Fail. 2014 Oct;2(5):457-65. doi: 10.1016/j.jchf.2014.05.007. Epub 2014 Sep 3. JACC Heart Fail. 2014. PMID: 25194287 Free PMC article. Clinical Trial.
-
The Role of Two Heart Biomarkers in IgA Nephropathy.Int J Mol Sci. 2023 Jun 19;24(12):10336. doi: 10.3390/ijms241210336. Int J Mol Sci. 2023. PMID: 37373483 Free PMC article.
References
-
- Fang J, Mensah GA, Croft JB, Keenan NL (2008) Heart failure-related hospitalization in the U.S., 1979 to 2004. J Am Coll Cardiol 52: 428–434. - PubMed
-
- Authors/Task Force Members, McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, et al. (2012) ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 14: 803–869. - PubMed
-
- Stewart S, MacIntyre K, Hole DJ, Capewell S, McMurray JJ (2001) More 'malignant' than cancer? Five-year survival following a first admission for heart failure. Eur J Heart Fail 3: 315–322. - PubMed
-
- Schou M, Gustafsson F, Videbaek L, Tuxen C, Keller N, et al... (2012) Extended heart failure clinic follow-up in low-risk patients: a randomized clinical trial (NorthStar). Eur Heart J. doi:10.1093/eurheartj/ehs235. - PubMed
-
- Komajda M, Lapuerta P, Hermans N, Gonzalez-Juanatey JR, van Veldhuisen DJ, et al. (2005) Adherence to guidelines is a predictor of outcome in chronic heart failure: the MAHLER survey. Eur Heart J 26: 1653–1659. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
