

Endovascular Management of Vascular Injury during Transsphenoidal Surgery
- PMID: 23472732
- PMCID: PMC3601607
- DOI: 10.1177/159101991301900116
Endovascular Management of Vascular Injury during Transsphenoidal Surgery
Abstract
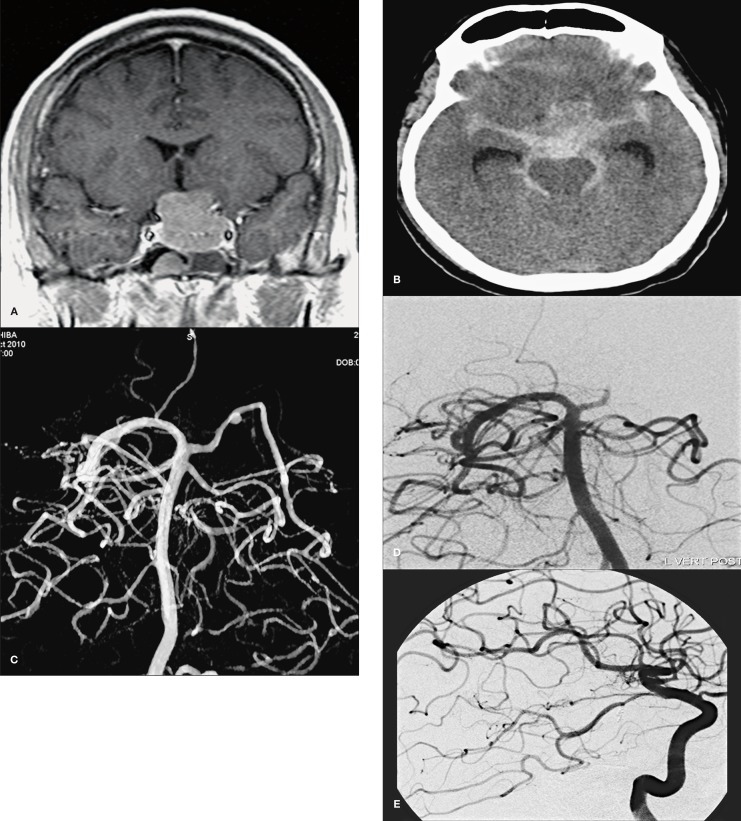
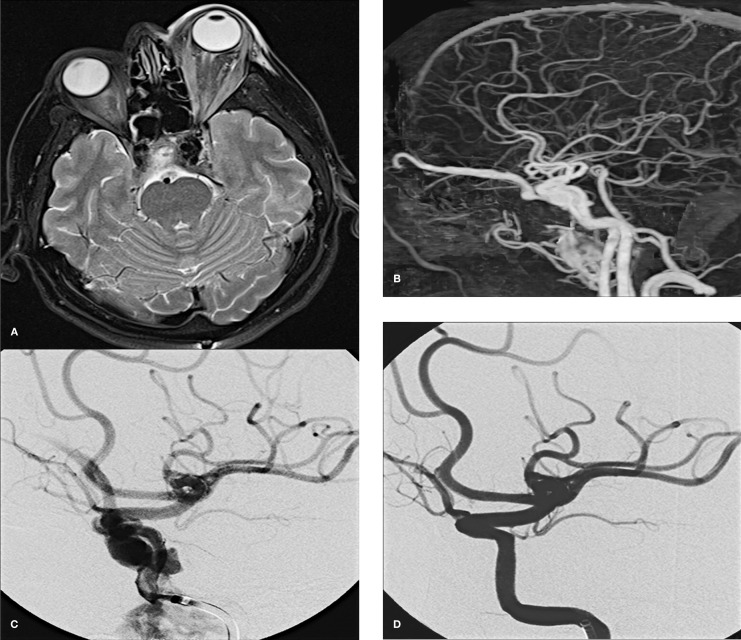
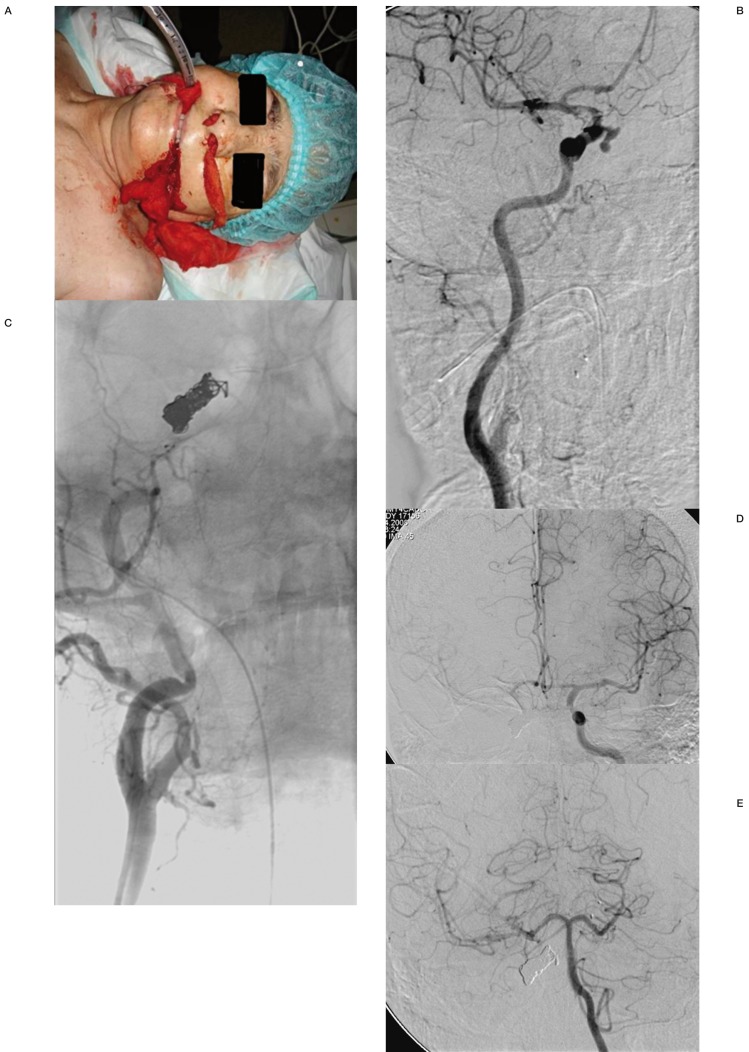
Vascular injury is an unusual and serious complication of transsphenoidal surgery. We aimed to define the role of angiography and endovascular treatment in patients with vascular injuries occurring during transsphenoidal surgery. During the last ten-year period, we retrospectively evaluated nine patients with vascular injury after transsphenoidal surgery. Eight patients were symptomatic due to vascular injury, while one had only suspicion of vascular injury during surgery. Four patients presented with epistaxis, two with subarachnoid hemorrhage, one with exophthalmos, and one with hemiparesia. Emergency angiography revealed a pseudoaneurysm in four patients, contrast extravasation in two, vessel dissection in one, vessel wall irregularity in one, and arteriovenous fistula in one. All patients but one were treated successfully with parent artery occlusion, with one covered stent implantation, one stent-assisted coiling method, while one patient was managed conservatively. One patient died due to complications related to the primary insult without rebleeding. Vascular injuries suspected intra or postoperatively must be investigated rapidly after transsphenoidal surgery. Endovascular treatment with parent artery occlusion is feasible with acceptable morbidity and mortality rates in the treatment of vascular injuries occurring in transsphenoidal surgery.
Figures
References
-
- Zervas NT. Surgical results for pituitary adenomas: results of an international survey. In: Black PMcL, Zervas NT, Ridgway EC, Jr, et al., editors. Secretory tumors of the pituitary gland. New York: Raven Press; 1984. pp. 377–385.
-
- Ahuja A, Guterman LR, Hopkins LN. Carotid cavernous fistula and false aneurysm of the cavernous carotid artery, complications of transsphenoidal surgery. Neurosurgery. 1992;31:774–778. - PubMed
-
- Ciric I, Ragin A, Baumgartner C, et al. Complications of transsphenoidal surgery results of a national survey, review of the literature, and personal experience. Neurosurgery. 1997;40:225–236. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
