

Clinical controversies: proton therapy for pediatric tumors
- PMID: 23473686
- PMCID: PMC3595134
- DOI: 10.1016/j.semradonc.2012.11.008
Clinical controversies: proton therapy for pediatric tumors
Abstract
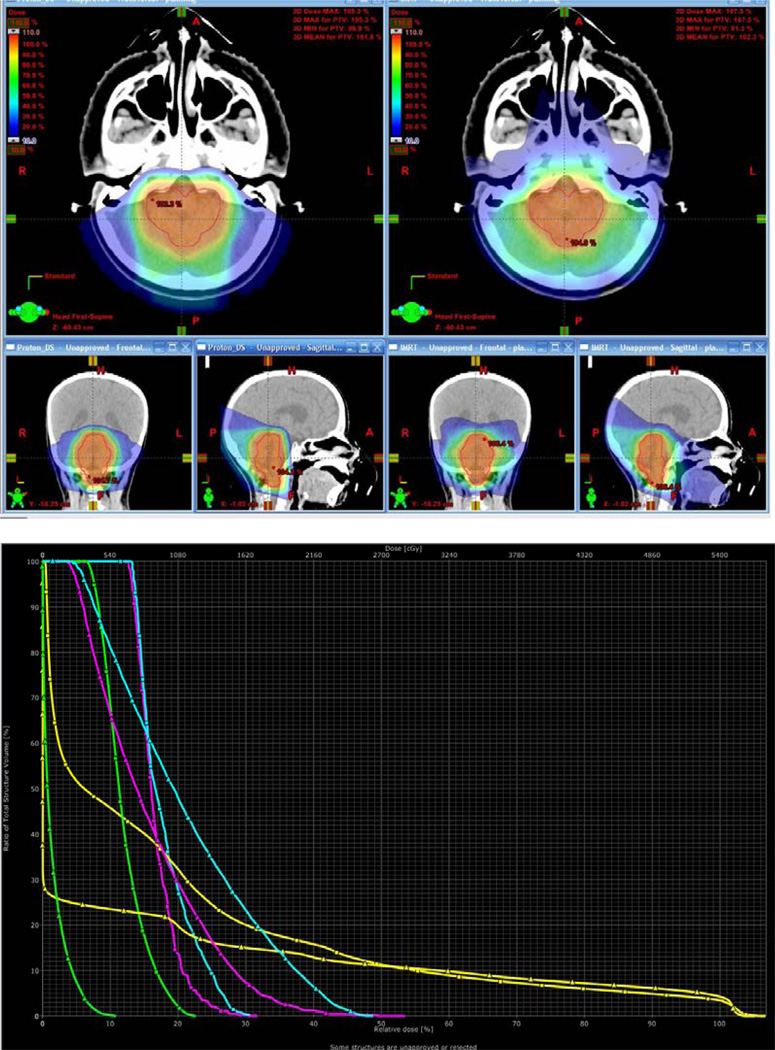
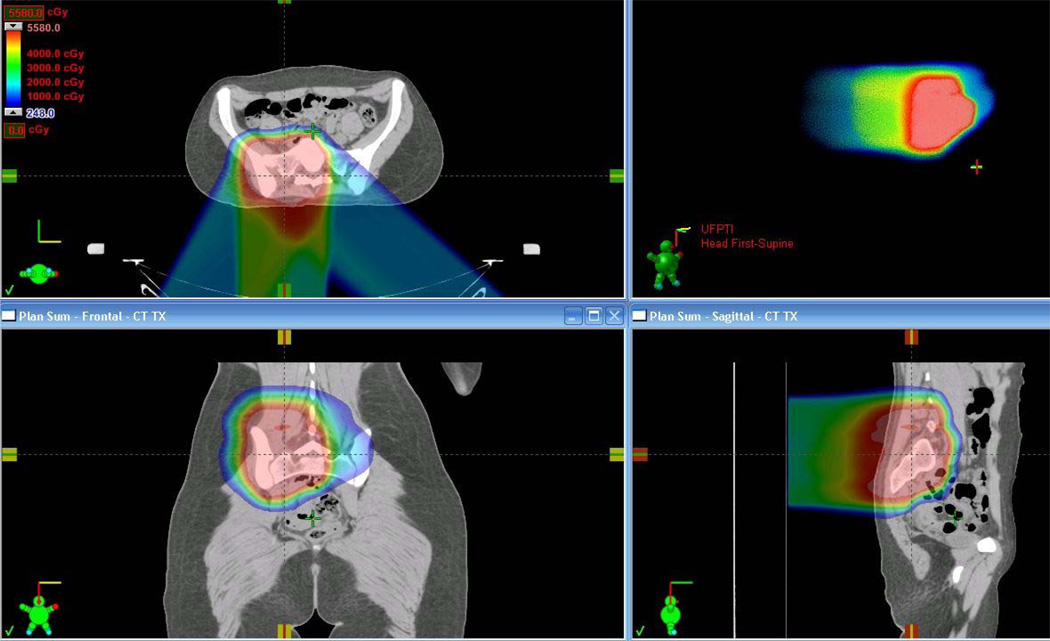
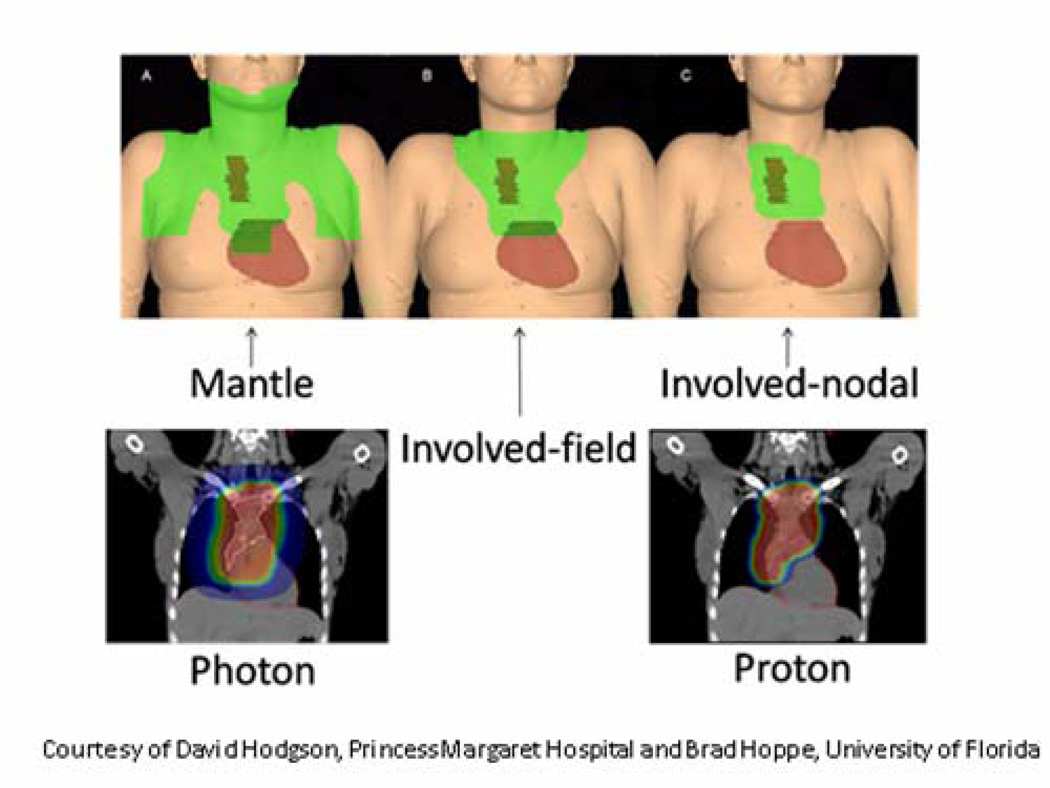
Despite the claim in the published literature, the introduction of proton therapy for children is not analogous to the evolution of conformal photon irradiation relying on the understanding of the impact of altered dose distributions. The differences in radiobiological effect when comparing photons with protons mean that we are comparing a known entity with an unknown entity: the dose-volume histogram for proton therapy might mean something substantially different from the dose-volume histogram for photon therapy. The multifaceted difference between the 2 modalities supports the argument for careful evaluation, follow-up, and clinical trials with adverse event monitoring when using proton therapy in children. We review the current data on the outcome of proton therapy in a range of pediatric tumors and compare them with the often excellent results of photon therapy in the setting of multidisciplinary management of childhood cancer. It is hoped that the apparent dosimetric advantage of proton therapy over photons will lead to improved indications for therapy, disease control, and functional outcomes. Although physical dose distribution is of clear importance, the multimodality management of children by an expert pediatric oncology team and the availability of ancillary measures that improve the quality of treatment delivery may be more important than the actual beam. In addition, current estimates of the benefit of proton therapy over photon therapy based on toxicity reduction will only be realized when survivorship has been achieved. Once substantive proton therapy data become available, it will be necessary to demonstrate benefit in clinically relevant outcome measures in comparison with best existing photon outcome data. Such an effort will require improved funding and appreciation for late effects research. Only real clinical outcome data combined with better understanding of the radiobiological differences between protons and photons will help us to further reduce side effects in children and exploit the full curative potential of this relatively new modality.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Laffond C, Dellatolas G, Alapetite C, et al. Quality-of-life, mood and executive functioning after childhood craniopharyngioma treated with surgery and proton beam therapy. Brain Inj. 2012;26:270–281. - PubMed
-
- Merchant TE, Kiehna EN, Kun LE, et al. Phase II trial of conformal radiation therapy for pediatric patients with craniopharyngioma and correlation of surgical factors and radiation dosimetry with change in cognitive function. J Neurosurg. 2006;104:94–102. - PubMed
-
- Rajan B, Ashley S, Thomas DG, et al. Craniopharyngioma: improving outcome by early recognition and treatment of acute complications. Int J Radiat Oncol Biol Phys. 1997;37:517–521. - PubMed
-
- Winkfield KM, Linsenmeier C, Yock TI, et al. Surveillance of craniopharyngioma cyst growth in children treated with proton radiotherapy. Int J Radiat Oncol Biol Phys. 2009;73:716–721. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
