

Next-generation sequencing: a powerful tool for the discovery of molecular markers in breast ductal carcinoma in situ
- PMID: 23477556
- PMCID: PMC3804339
- DOI: 10.1586/erm.13.4
Next-generation sequencing: a powerful tool for the discovery of molecular markers in breast ductal carcinoma in situ
Abstract
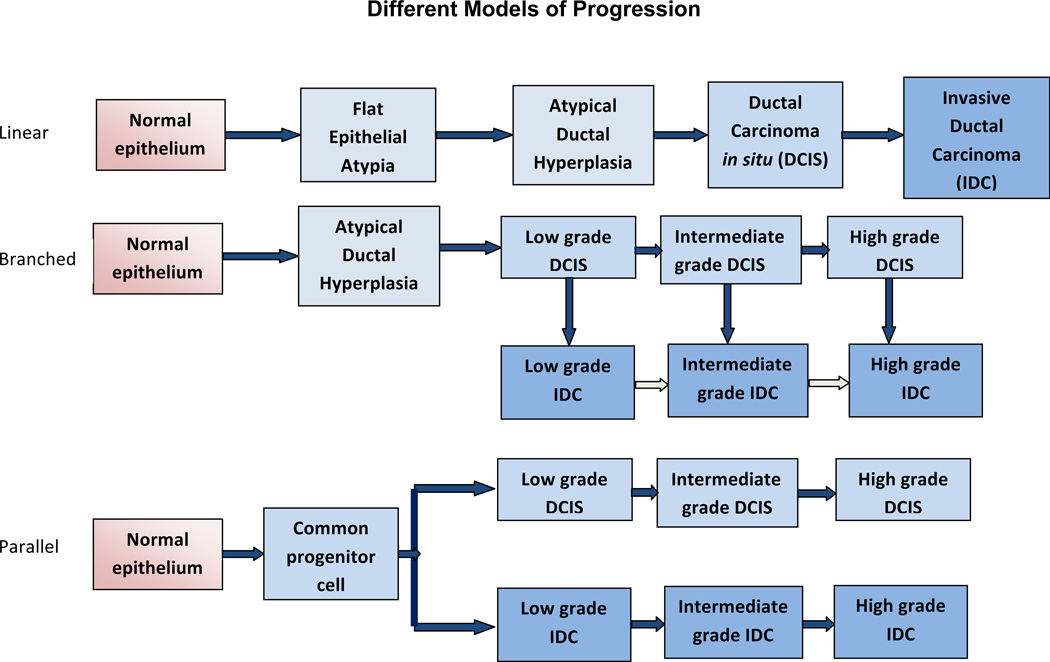
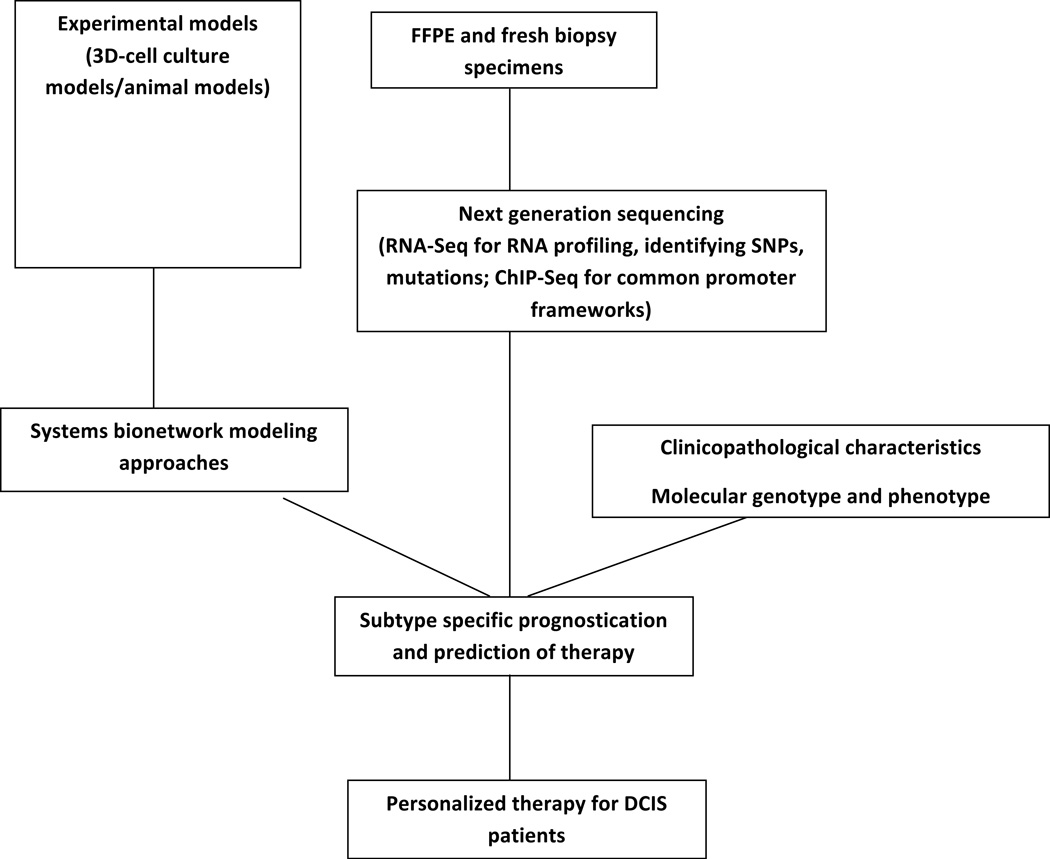
Mammographic screening leads to frequent biopsies and concomitant overdiagnosis of breast cancer, particularly ductal carcinoma in situ (DCIS). Some DCIS lesions rapidly progress to invasive carcinoma, whereas others remain indolent. Because we cannot yet predict which lesions will not progress, all DCIS is regarded as malignant, and many women are overtreated. Thus, there is a pressing need for a panel of molecular markers in addition to the current clinical and pathological factors to provide prognostic information. Genomic technologies such as microarrays have made major contributions to defining subtypes of breast cancer. Next-generation sequencing (NGS) modalities offer unprecedented depth of expression analysis through revealing transcriptional boundaries, mutations, rare transcripts and alternative splice variants. NGS approaches are just beginning to be applied to DCIS. Here, the authors review the applications and challenges of NGS in discovering novel potential therapeutic targets and candidate biomarkers in the premalignant progression of breast cancer.
Conflict of interest statement
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. This review was written solely by the authors without any additional writing assistance.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA: a cancer journal for clinicians. 2012;62(1):10–29. - PubMed
-
- Tabar L, Vitak B, Chen HH, Yen MF, Duffy SW, Smith RA. Beyond randomized controlled trials: organized mammographic screening substantially reduces breast carcinoma mortality. Cancer. 2001;91(9):1724–1731. - PubMed
-
- Kopans DB. Just the facts: mammography saves lives with little if any radiation risk to the mature breast. Health Phys. 2011;101(5):578–582. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical