

Effects of azithromycin in Pseudomonas aeruginosa burn wound infection
- PMID: 23478086
- PMCID: PMC3713079
- DOI: 10.1016/j.jss.2013.02.003
Effects of azithromycin in Pseudomonas aeruginosa burn wound infection
Abstract
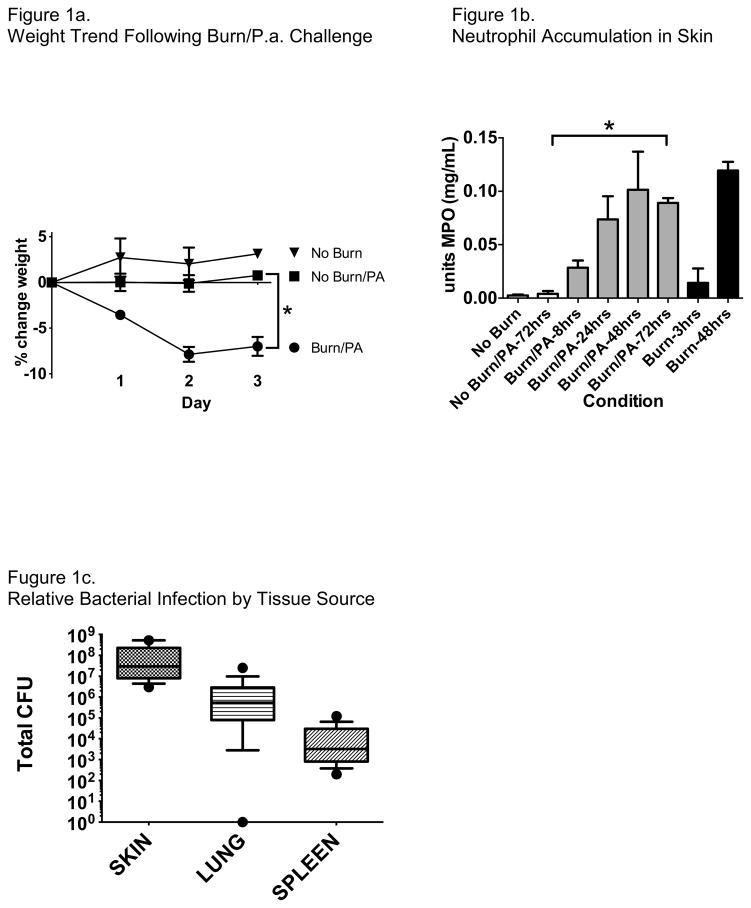
Background: Cutaneous thermal injuries (i.e., burns) remain a common form of debilitating trauma, and outcomes are often worsened by wound infection with environmental bacteria, chiefly Pseudomonas aeruginosa.
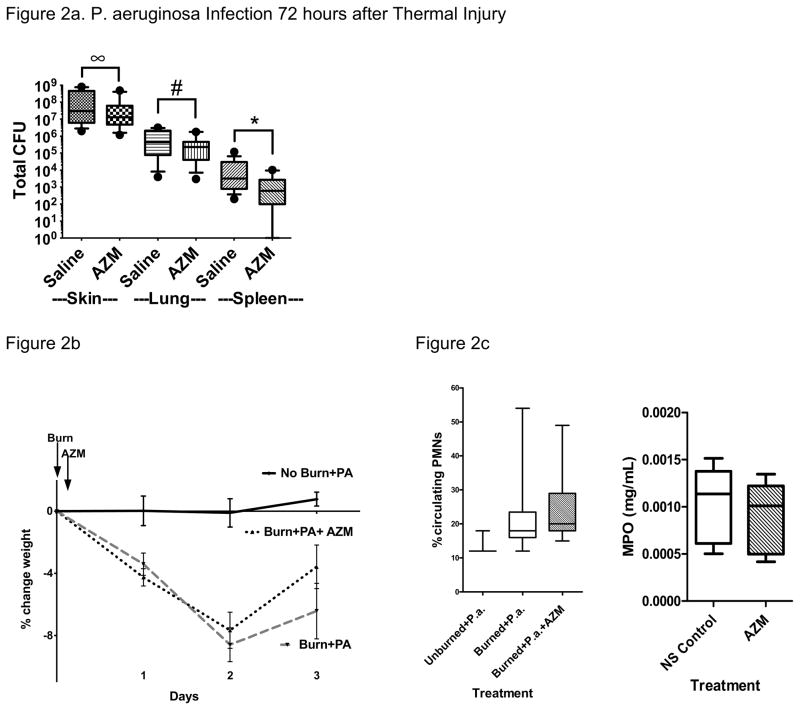
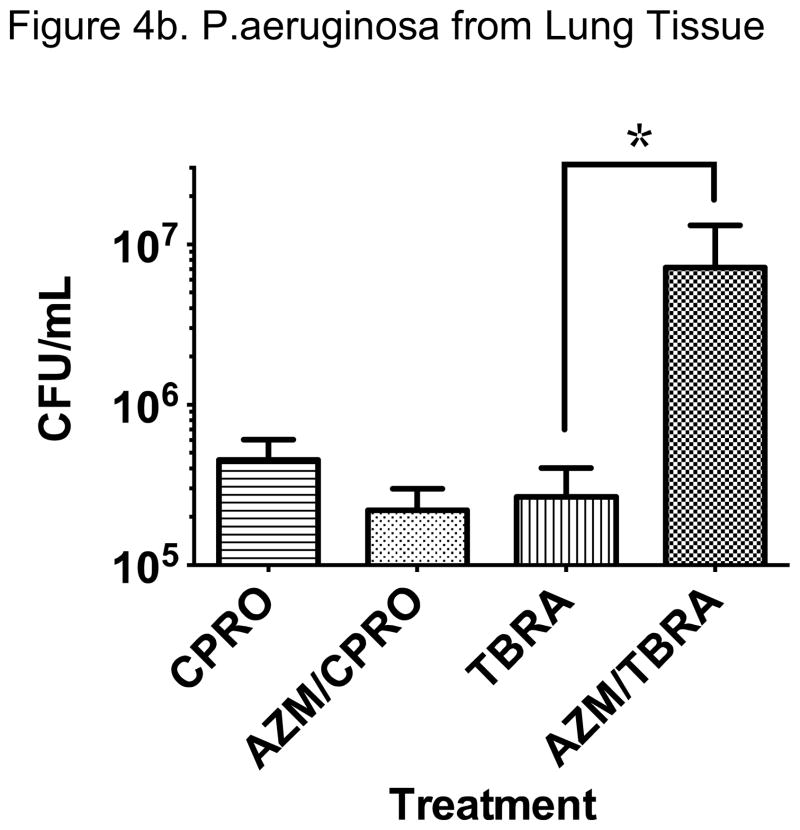
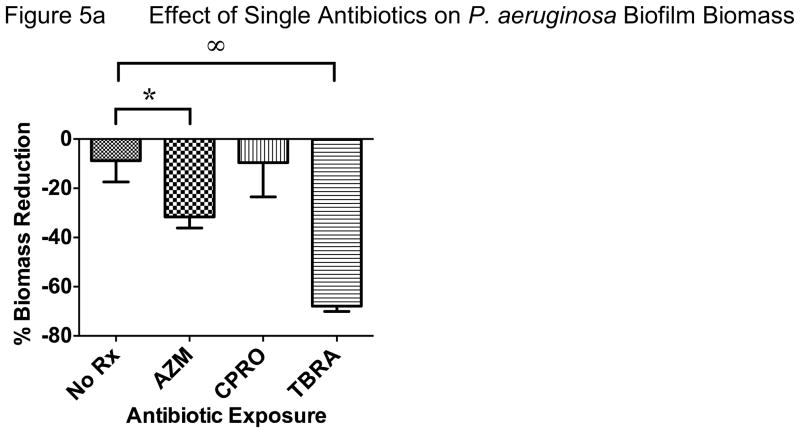
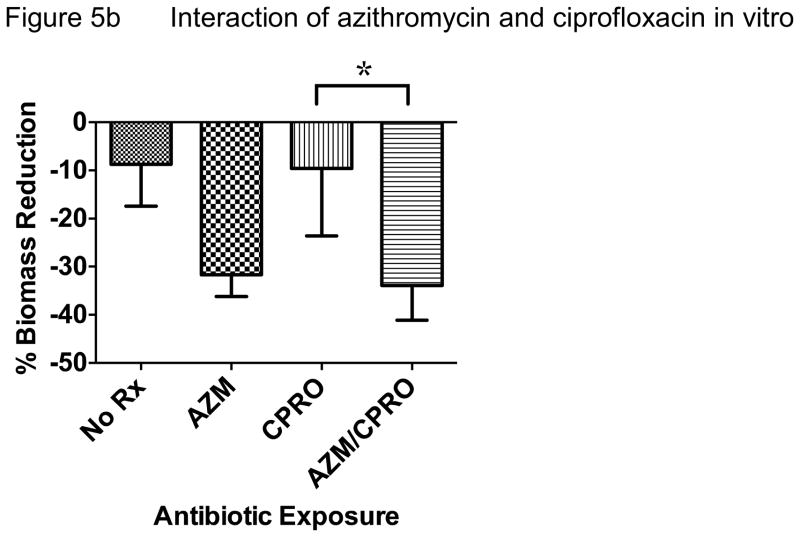
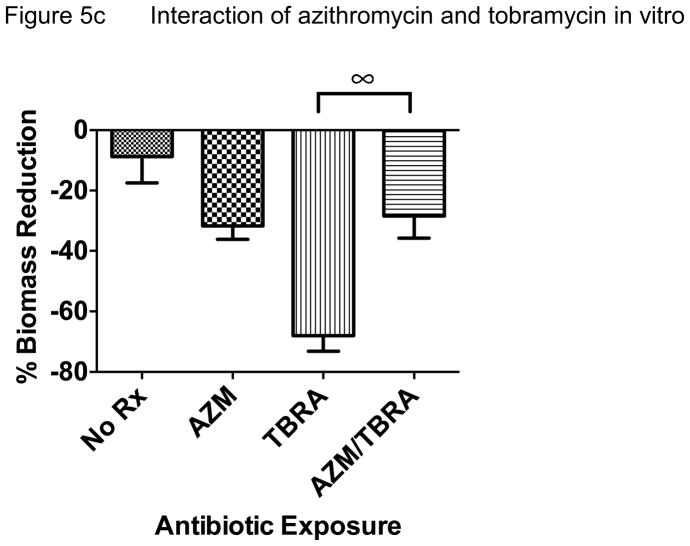
Materials and methods: We tested the effects of early administration of a single dose of azithromycin, with or without subsequent antipseudomonal antibiotics, in a mouse model of standardized thermal injury infected with P aeruginosa via both wound site and systemic infection. We also tested the antimicrobial effects of these antibiotics alone or combined in comparative biofilm and planktonic cultures in vitro.
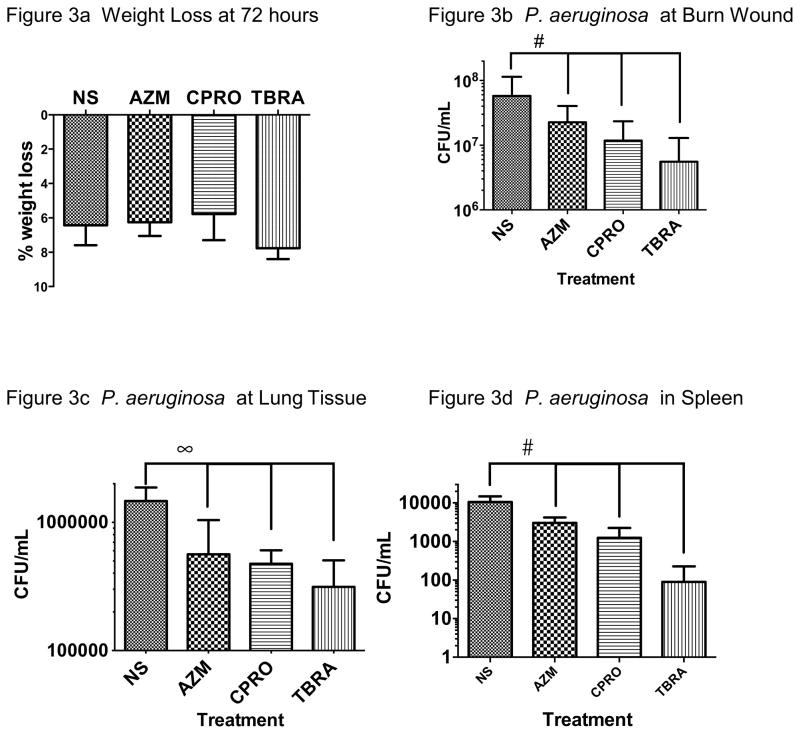
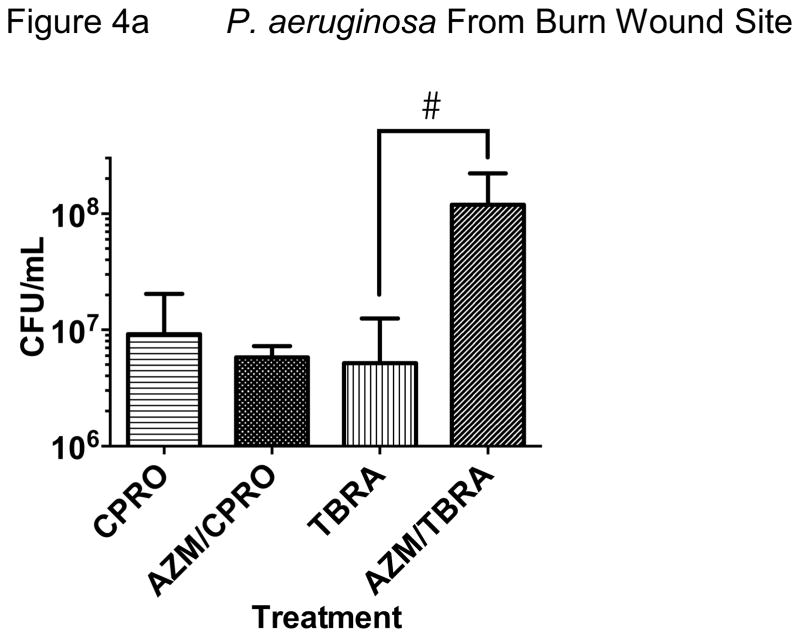
Results: In our model, early azithromycin administration significantly reduced wound and systemic infection without altering wound site or circulating neutrophil activity. The antimicrobial effect of azithromycin was additive with ciprofloxacin but significantly reduced the antimicrobial effect of tobramycin. This pattern was reproduced in biofilm cultures and not observed in planktonic cultures of P aeruginosa.
Conclusion: These data suggest that early administration of azithromycin following burn-related trauma and infection may reduce P aeruginosa infection and potential interactions with other antibiotics should be considered when designing future studies.
Keywords: Azithromycin; Biofilm; Burn; Burn wound; Ciprofloxacin; Cystic fibrosis; Drug–drug interaction; Pseudomonas aeruginosa; Thermal injury; Tobramycin.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
References
-
- Burn incidence and treatment in the united states: 2011 Fact Sheet. American burn association; 2011.
-
- Roeder RA, Schulman CI. An Overview of war-related thermal injuries. J Craniofac Surg. 2010;21:971–975. - PubMed
-
- Mayhall CG. The epidemiology of burn wound infections: then and now. Clin Infect Dis. 2003;37(4):543–550. - PubMed
-
- Baker CC, Miller CL, Trunkey DD. Predicting fatal sepsis in burn patients. J Trauma. 1979;19(9):641–648. - PubMed
-
- Barrow RE, Spies M, Barrow LN, Herndon DN. Influence of demographics and inhalation injury on burn mortality in children. Burns. 2004;30(1):72–77. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
