

Determinants of successful glycemic control among participants in the BARI 2D trial: a post-hoc analysis
- PMID: 23478173
- PMCID: PMC4156479
- DOI: 10.1016/j.jdiacomp.2013.01.006
Determinants of successful glycemic control among participants in the BARI 2D trial: a post-hoc analysis
Abstract
Objective: The BARI 2D trial compared insulin provision (IP) versus insulin sensitization (IS) for the primary outcome of total mortality in participants with T2DM and cardiovascular disease (CVD). In this analysis we examine baseline characteristics that are associated with successful long-term glycemic control.
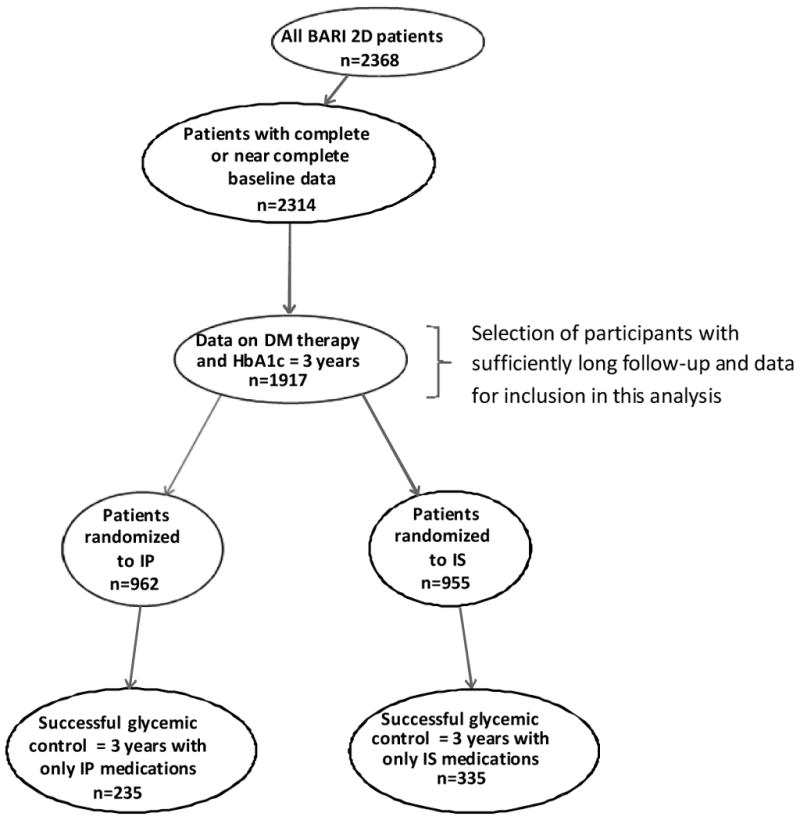
Research design and methods: In a 2×2 factorial design, 2368 participants were randomized to either IP or IS therapy, and to either prompt revascularization with medical therapy or medical therapy alone. Successful long-term glycemic control (success) was defined by simultaneously meeting 1) a mean HbA1c level of <7.0% after each participant's third year of follow-up period, and 2) adherence with medications only from the assigned glycemic treatment arm during >80% of the BARI 2D follow-up. The association between baseline variables and success was determined using unadjusted and adjusted logistic regression models.
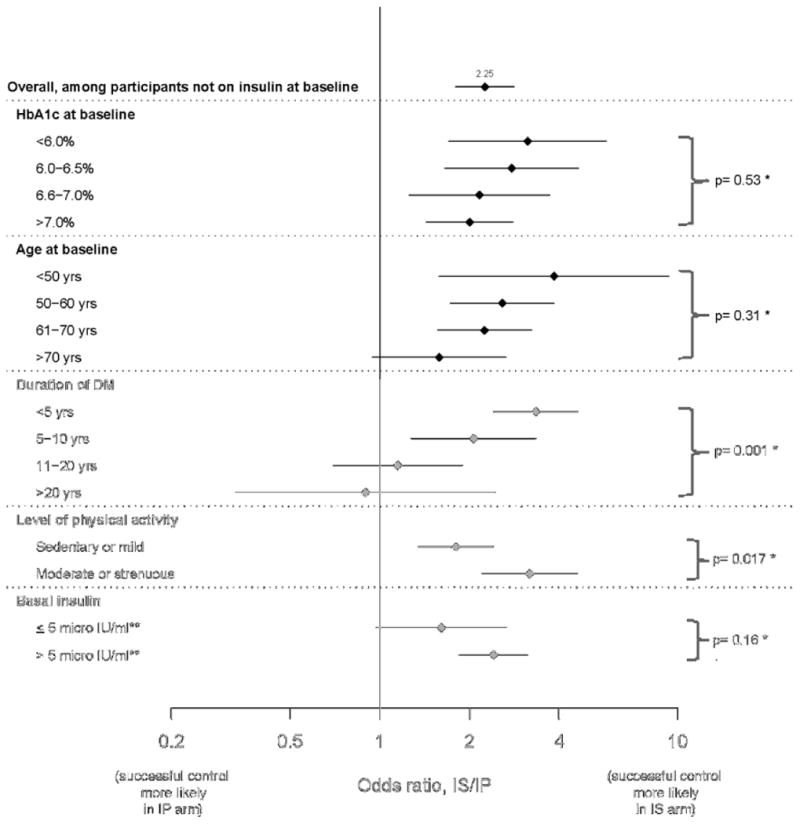
Results: 1917 participants (962 IP and 955 IS participants) had sufficiently long follow-up and data for this analysis. Among these IP and IS participants, 235 and 335 participants met both criteria of success, respectively (p<0.001). Those not on insulin at entry had higher odds of success (OR 2.25; CI 1.79-2.82) when treated with IS versus IP medications, irrespective of baseline HbA1c levels. Younger age, shorter duration of T2DM, and lower HbA1c at baseline were also each independently associated with higher success when treated with IS versus IP medications.
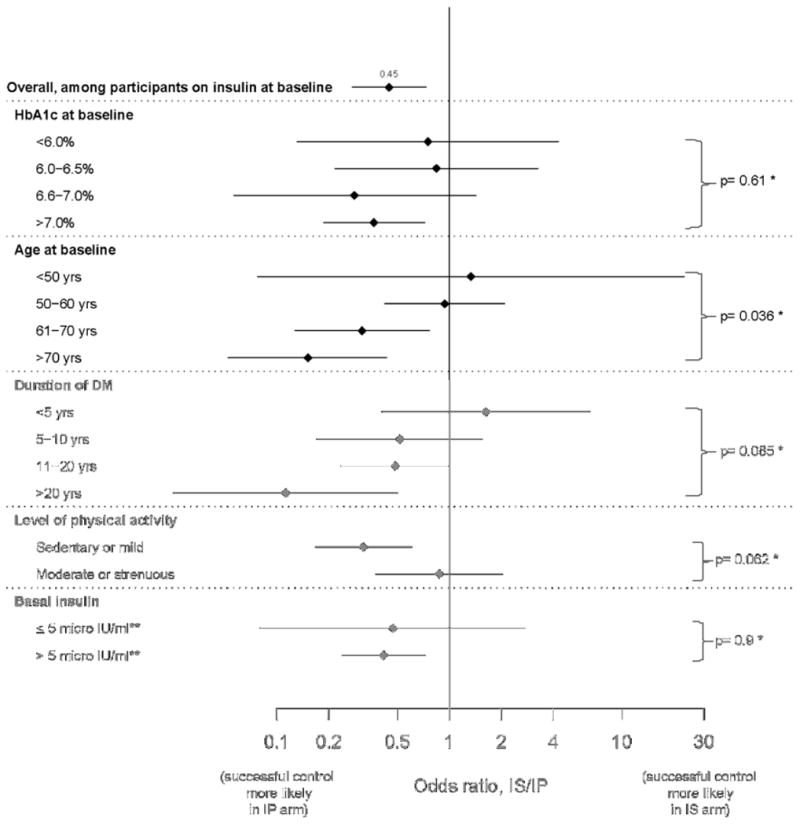
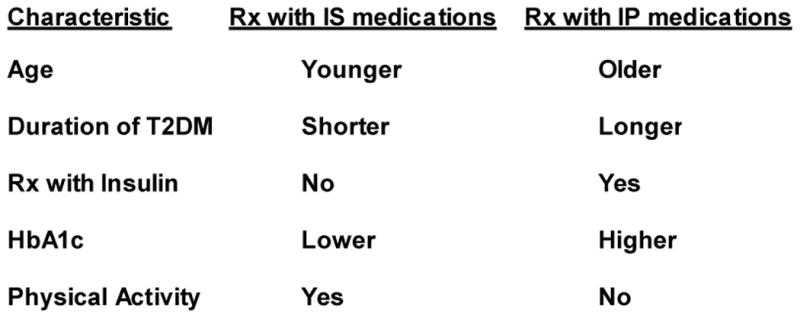
Conclusion: Patients similar to those in the BARI 2D trial may have a higher chance of achieving success with IS versus IP medications if they are younger, have shorter duration of T2DM, have lower HbA1c levels, have moderate or strenuous physically activity, and are not on insulin. In contrast, increasing age, longer duration of T2DM, higher HbA1c, and insulin therapy are associated with increased chance of success if treated with IP medications.
Keywords: Cardiovascular disease; Plasma insulin levels; Predictors of glycemic control.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
References
-
- Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HAW. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. N Engl J Med. 2008;359:1577–1589. - PubMed
-
- Skyler JS, Bergenstal R, Bonow RO, Buse J, Deedwania P, Gale EAM, Howard BV, Kirkman MS, Kosiborod M, Reaven P, Sherwin RS. Intensive glycemic control and the prevention of cardiovascular events: Implications of the ACCORD, ADVANCE, and VA Diabetes Trials. A position statement of the American Diabetes Association and a scientific statement of the American College of Cardiology Foundation and the American Heart Association. Circulation. 2009;119:351–357. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
