

Optimal selection of asymptomatic patients for carotid endarterectomy based on predicted 5-year survival
- PMID: 23478502
- PMCID: PMC3930459
- DOI: 10.1016/j.jvs.2012.12.056
Optimal selection of asymptomatic patients for carotid endarterectomy based on predicted 5-year survival
Abstract
Objective: Although carotid endarterectomy (CEA) is performed to prevent stroke, long-term survival is essential to ensure benefit, especially in asymptomatic patients. We examined factors associated with 5-year survival following CEA in patients with asymptomatic internal carotid artery (ICA) stenosis.
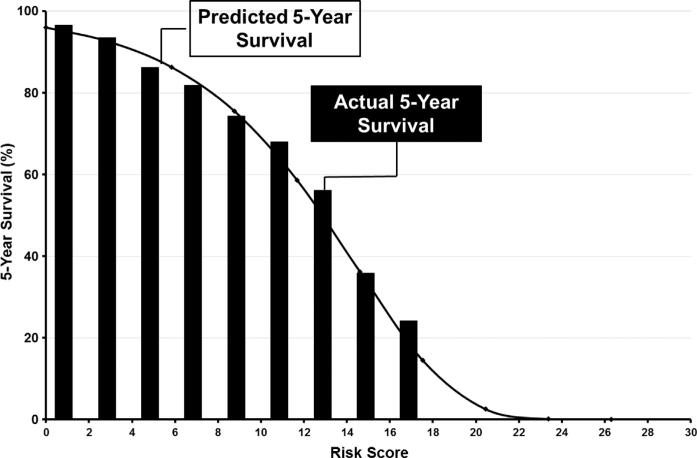
Methods: Prospectively collected data from 4114 isolated CEAs performed for asymptomatic stenosis across 24 centers in the Vascular Study Group of New England between 2003 and 2011 were used for this analysis. Late survival was determined with the Social Security Death Index. Cox proportional hazard models were used to identify risk factors for mortality within the first 5 years after CEA and to calculate a risk score for predicting 5-year survival.
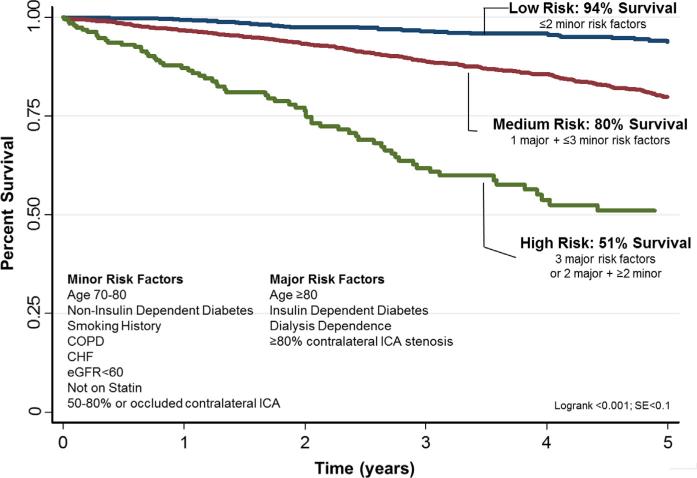
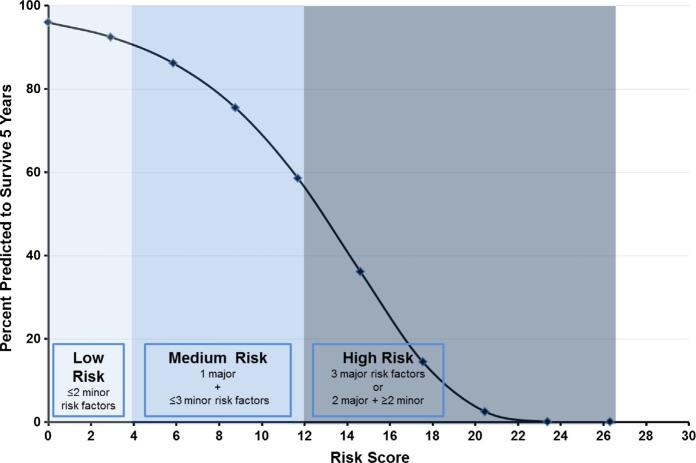
Results: Overall 3- and 5-year survival after CEA in asymptomatic patients were 90% (95% CI 89%-91%) and 82% (95% CI 81%-84%), respectively. By multivariate analysis, increasing age, diabetes, smoking history, congestive heart failure, chronic obstructive pulmonary disease, poor renal function (estimated glomerular filtration rate <60 or dialysis dependence), absence of statin use, and worse contralateral ICA stenosis were all associated with worse survival. Patients classified as low (27%), medium (68%), and high risk (5%) based on number of risk factors had 5-year survival rates of 96%, 80%, and 51%, respectively (P < .001).
Conclusions: More than four out of five asymptomatic patients selected for CEA in the Vascular Study Group of New England achieved 5-year survival, demonstrating that, overall, surgeons in our region selected appropriate patients for carotid revascularization. However, there were patients selected for surgery with high risk profiles, and our models suggest that the highest risk patients (such as those with multiple major risk factors including age ≥ 80, insulin-dependent diabetes, dialysis dependence, and severe contralateral ICA stenosis) are unlikely to survive long enough to realize a benefit of prophylactic CEA for asymptomatic stenosis. Predicting survival is important for decision making in these patients.
Copyright © 2013 Society for Vascular Surgery. All rights reserved.
Figures
Comment in
-
Discussion.J Vasc Surg. 2013 Jul;58(1):118-9. doi: 10.1016/j.jvs.2012.12.086. Epub 2013 Mar 7. J Vasc Surg. 2013. PMID: 23478506 No abstract available.
-
Invited commentary.J Vasc Surg. 2013 Jul;58(1):119. doi: 10.1016/j.jvs.2013.01.004. J Vasc Surg. 2013. PMID: 23806254 No abstract available.
References
-
- Agency for Healthcare Research and Quality [November 2011]; Available at: http://www.ahrq.gov/data/hcup.
-
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991;325:445–53. - PubMed
-
- Chaturvedi S. Public health impact of carotid endarterectomy. Neuroepidemiology. 1999;18:15–21. - PubMed
-
- Abbott AL. Medical (nonsurgical) intervention alone is now best for prevention of stroke associated with asymptomatic severe carotid stenosis: results of a systematic review and analysis. Stroke. 2009;40:e573–83. - PubMed
-
- Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA. 1995;273:1421–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
