

Comparative effectiveness of inhospital trauma resuscitation at a French trauma center and matched patients treated in the United States
- PMID: 23478519
- PMCID: PMC3989531
- DOI: 10.1097/SLA.0b013e31828226b6
Comparative effectiveness of inhospital trauma resuscitation at a French trauma center and matched patients treated in the United States
Abstract
Objective: The objective of this paper is to compare mortality outcomes between patients treated at a trauma center in France and matched patients in the United States.
Background: Although trauma systems in France and the United States differ significantly in prehospital and inhospital management, previous comparisons have been challenged by the lack of comparable data.
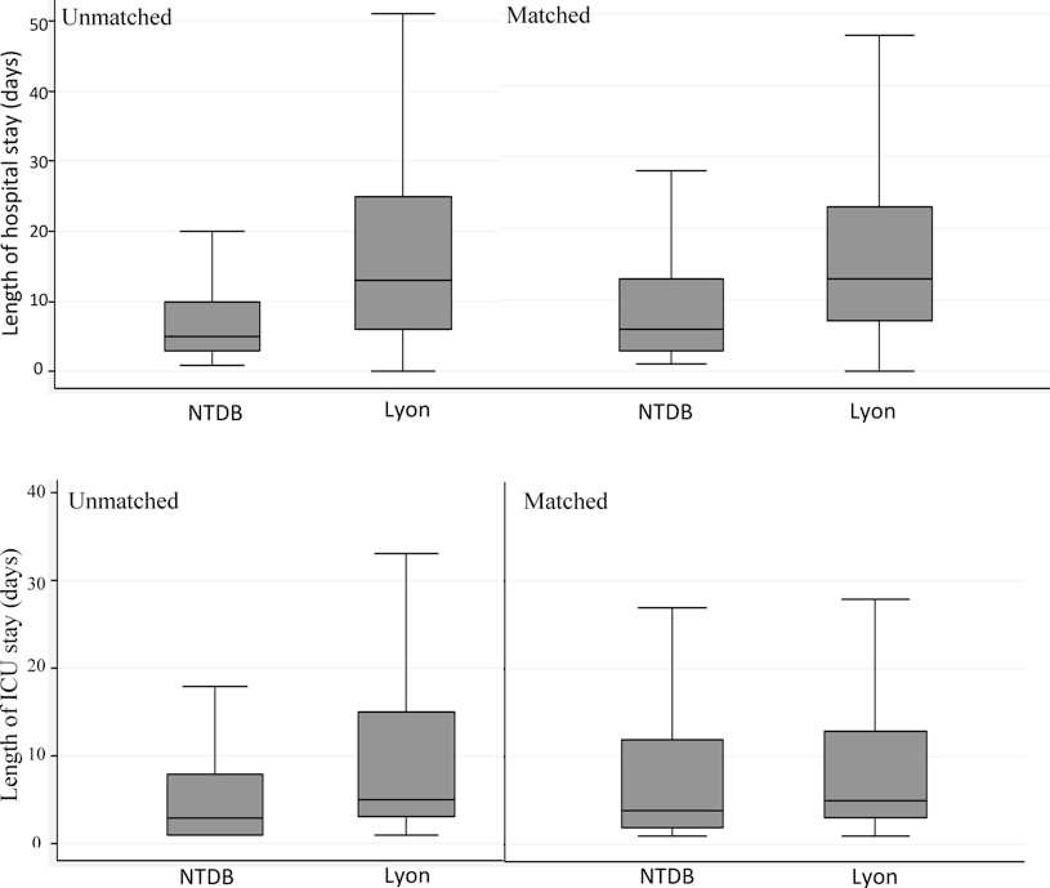
Methods: Coarsened exact matching identified matching patients between a single center trauma database from Lyon, France, and the National Trauma Data Bank (NTDB) of the United States. Moderate to severely injured [injury severity score (ISS) > 8] adult patients (age ≥ 16) presenting alive to level 1 trauma centers from 2002 to 2005 with blunt or penetrating injuries were included. After matching patients, multivariate regression analyses were performed to determine difference in mortality between patients in Lyon and the NTDB.
Results: A total of 1043 significantly injured patients were presented to the Lyon center. Matching eligible patients with complete records were sought from 219,985 patients in the NTDB. The unadjusted odds of mortality at the Lyon center was 2.5 times higher than that of the NTDB [95% confidence interval (CI) = 2.18-2.98]. However, the Lyon center received patients with higher ISS, lower Glasgow Coma Score (GCS), and lower systolic blood pressure (SBP) (all P < 0.001). After 1:1 matching, 858 patient pairs were produced, and the odds of mortality became equivalent [odds ratio (OR) = 1.3, 95% CI = 0.91-1.73]. Similar results were found in multiple subset analyses.
Conclusions: Trauma patients admitted to a single French trauma center had an equal chance of survival compared with similarly injured patients treated at US trauma centers.
Conflict of interest statement
None of the authors has any conflicts of interest.
Figures

Comment in
-
Is Field Resuscitation by Nonsurgeons Equivalent to In-hospital Resuscitation by Trauma Surgeons?Ann Surg. 2015 Jul;262(1):e29. doi: 10.1097/SLA.0000000000000618. Ann Surg. 2015. PMID: 24646538 No abstract available.
References
-
- World Health Organization. Disease and injury country estimates. 2004 [updated 2004; cited 2011 June 26]; Available from: http://apps.who.int/ghodata/
-
- Nathens AB, Brunet FP, Maier RV. Development of trauma systems and effect on outcomes after injury. Lancet. 2004 May 29;363(9423):1794–1801. - PubMed
-
- Dick WF. Anglo-American vs. Franco-German emergency medical services system. Prehosp Disaster Med. 2003 Jan-Mar;18(1):29–35. discussion-7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
