

Temporal trends in treatment and outcomes for advanced heart failure with reduced ejection fraction from 1993-2010: findings from a university referral center
- PMID: 23479563
- PMCID: PMC3674961
- DOI: 10.1161/CIRCHEARTFAILURE.112.000178
Temporal trends in treatment and outcomes for advanced heart failure with reduced ejection fraction from 1993-2010: findings from a university referral center
Abstract
Background: Randomized trials have demonstrated the efficacy of several new therapies for heart failure (HF) with reduced ejection fraction over the preceding 2 decades. This study investigates whether these therapeutic advances have translated into improvement in outcomes for patients with advanced HF referred to a heart transplant center.
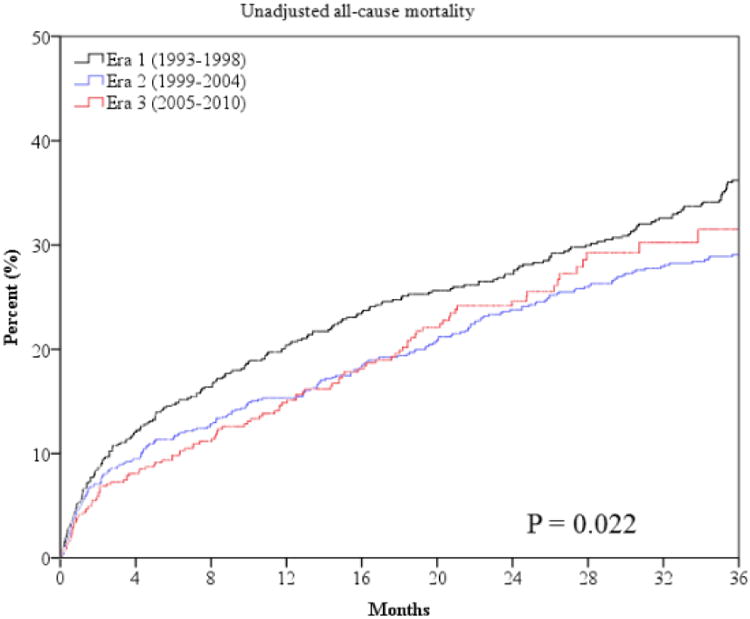
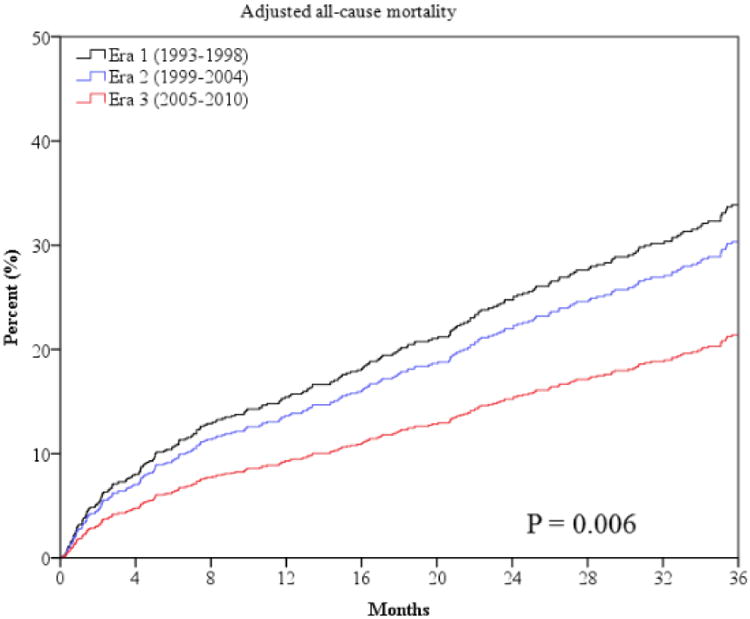
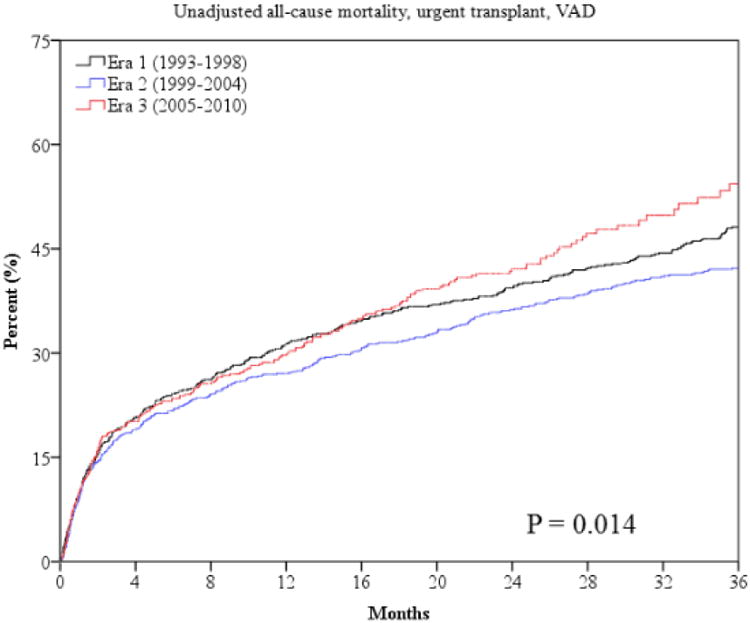
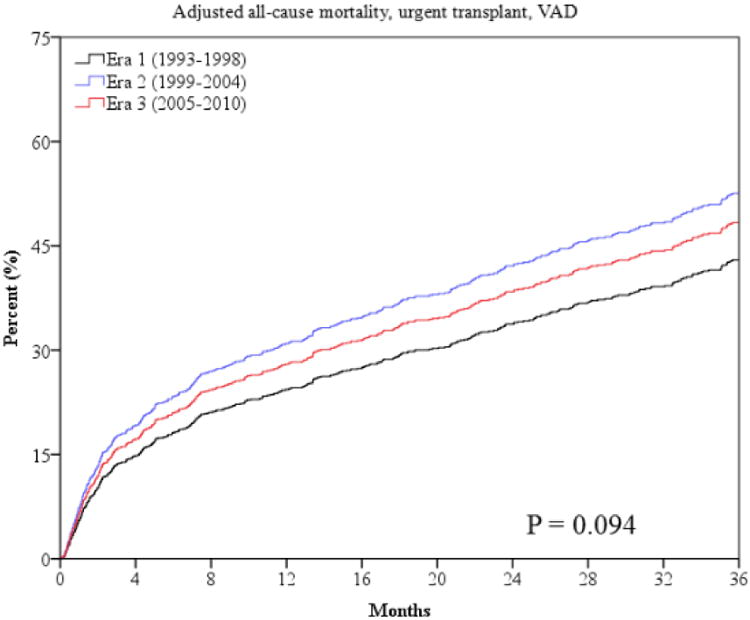
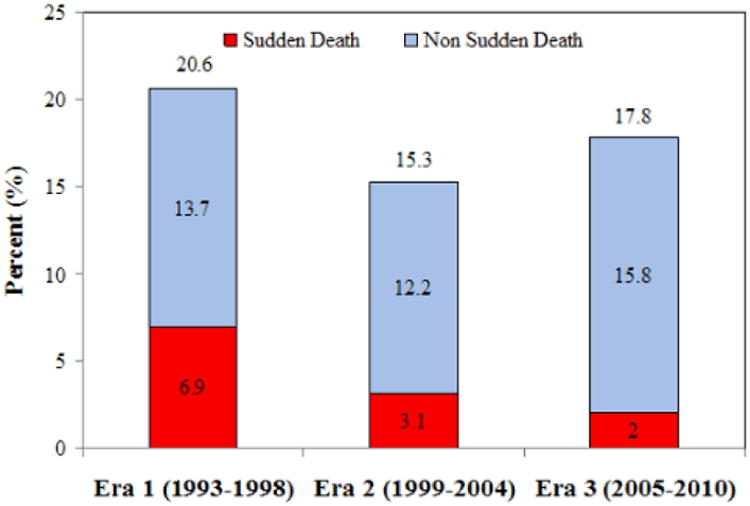
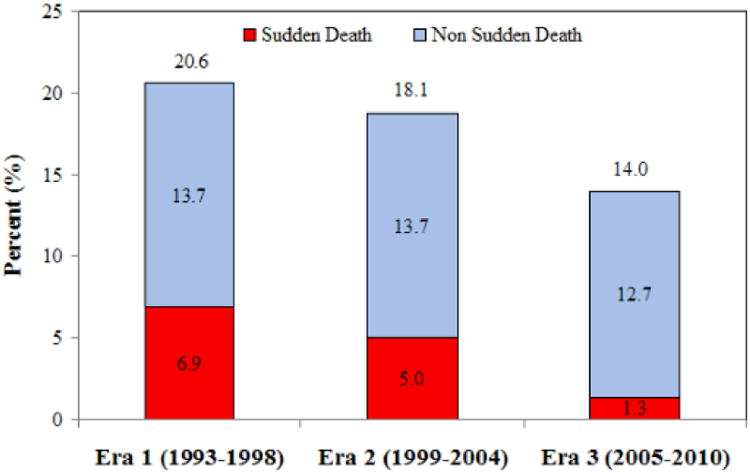
Methods and results: Patients with HF (n=2507) referred to a single university center were analyzed in three 6-year eras during which medical and device therapies were evolving: 1993 to 1998 (era 1), 1999 to 2004 (era 2), and 2005 to 2010 (era 3). Impaired hemodynamics and comorbidities were more frequent at time of referral in later eras, whereas other HF severity parameters where similar or improved. Successive eras had greater usage of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, β-blockers, aldosterone antagonists, implantable cardioverter defibrillators, and cardiac resynchronization therapy, consistent with evolving evidence and guideline recommendations over the study period. All-cause mortality and sudden death were significantly lower in era 2 and 3 compared with era 1. After multivariable risk adjustment, era 3 had significantly decreased 2- and 3-year all-cause mortality risk and significantly decreased 1- and 3-year sudden death risk compared with era 1. However, progressive HF death and the combined outcome of mortality/urgent transplant/ventricular assist device were modestly increased in the latter eras.
Conclusions: Over the past 2 decades, patients with advanced HF referred to and managed at a tertiary university referral center have benefited from advances in HF medications and devices, as evidenced by improvements in overall survival and sudden death risk.
Keywords: heart failure; mortality; therapy.
Figures
Comment in
-
Diff'rent strokes, different folks: advanced heart failure's changing outlook.Circ Heart Fail. 2013 May;6(3):355-7. doi: 10.1161/CIRCHEARTFAILURE.113.000285. Circ Heart Fail. 2013. PMID: 23694769 Free PMC article. No abstract available.
References
-
- Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, Konstam MA, Mancini DM, Rahko PS, Silver MA, Stevenson LW, Yancy CW. ACCF/AHA guidelines for the diagnosis and management of heart failure in adults. Circulation. 2009;119:1977–2016. - PubMed
-
- SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med. 1991;325:293–302. - PubMed
-
- Hjalmarson Å, Goldstein S, Fagerberg B, Wedel H, Waagstein F, Kjekshus J, Wikstrand J, El Allaf D, Vítovec J, Aldershvile J, Halinen M, Dietz R, Neuhaus KL, Jánosi A, Thorgeirsson G, Dunselman PH, Gullestad L, Kuch J, Herlitz J, Rickenbacher P, Ball S, Gottlieb S, Deedwania P. Effects of controlled-release metoprolol on total mortality, hospitalizations, and well-being in patients with heart failure. JAMA. 2000;283:1295–1302. - PubMed
-
- Poole-Wilson PA, Swedberg K, Cleland JGF, Di Lenarda A, Hanrath P, Komajda M, Lubsen J, Lutiger B, Metra M, Remme WJ, Torp-Pedersen C, Scherhag A, Skene A. Comparison of carvedilol and metoprolol on clinical outcomes in patients with chronic heart failure in the Carvedilol or Metoprolol European Trial (COMET): randomised controlled trial. Lancet. 2003;362:7–13. - PubMed
-
- Pfeffer MA, Braunwald E, Moyé LA, Basta L, Brown EJ, Cuddy TE, Davis BR, Geltman EM, Goldman S, Flaker GC, Klein M, Lamas GA, Packer M, Rouleau J, Rouleau JL, Rutherford J, Wertheimer JH, Hawkins CM. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 1992;327:669–677. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
